



Winning patients for life is not difficult. The ELZA Institute, where I practice, uses several strategies to attract and retain patients. What may surprise you is that social media doesn’t play a big role in our efforts. The essential strategic elements are a solid knowledge base, sincerity, and empathy.
A large portion of our patients have keratoconus. Dozens of people present each month with all stages of the disease. Keratoconus disproportionately affects children and adolescents, but it can affect people of all ages (Figure 1).1 If the disease is not treated in a timely fashion, corneal steepening and thinning typically result in significant visual impairment.
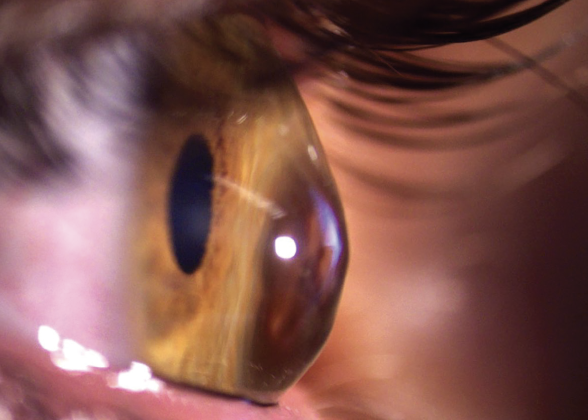
Figure 1. The eye of a middle-aged patient with advanced keratoconus and an intolerance of contact lenses.
Our relationships with patients—particularly those with keratoconus—often lasts many years. Establishing trust and an empathic connection is the key to maintaining these relationships for the long term.
PROVIDE EDUCATION WITH EMPATHY AND COMPASSION
Children and young adults with keratoconus are typically accompanied by their parents, guardians, or other family members. All of them are anxious about their diagnosis and worried about what comes next. They are generally confused and overwhelmed because the treatment strategy can be complex and vary by disease stage and the age of the patient.
Most important is to inform and reassure everyone involved that treatment options are available that address the spectrum of the disease—from its earliest, subclinical forms to its advanced stages. It’s also important to explain that there are two aspects of treatment: halting disease progression and rehabilitating vision.
Demonstrating empathy and compassion during discussions builds trust between the patient, their family, you, and your team and forms the foundation of a positive and long-lasting relationship.
MANAGING EXPECTATIONS
Managing patient expectations and being clear about their responsibilities are important to the doctor-patient relationship. For children with keratoconus, the high likelihood (77%–88%) of disease progression without treatment means that they and their families must be informed that CXL should be performed shortly after diagnosis unless there is a strong reason against it.2,3 It’s also essential to educate them that eye rubbing exacerbates the disease4 and that concomitant ocular diseases such as allergies can worsen symptoms and require treatment.5
Systemic diseases and conditions can also influence keratoconus progression, particularly in older patients. Conditions such as pregnancy that result in dysregulations in hormone homeostasis (eg, estrogen6 or thyroid7) can hasten disease progression. In contrast, diabetes, smoking,8 and aging9 tend to protect against disease progression.7,10
Clearly communicate the risks and how best to manage them, including the importance of follow-up visits.
KEEP IT REAL
When speaking with patients and their families, be open and honest about the disease, its treatment, and the prospect of visual rehabilitation. A mantra in the refractive surgery field is to underpromise and overdeliver. It is also important to offer hope.
Many patients with keratoconus or similar forms of ectasia can benefit from visual rehabilitation, typically with scleral or rigid gas permeable contact lenses. In some instances—usually older patients with stable disease and sufficiently thick corneas—therapeutic excimer laser surgery can be beneficial. When possible, reassure patients that their situation can improve.
A patient of mine with keratoglobus and a cornea that was approximately 200 µm thick underwent CXL using a novel protocol called sub400 (Figure 2).11,12 His ectasia has been stable and his visual acuity with scleral contact lenses satisfactory for the 3 years since he underwent intervention. Two or three years before he received treatment, CXL would not have been possible because of his thin corneas. I share this case to illustrate that there is always hope that what isn’t possible today may be possible tomorrow.

Figure 2. Recent advances in CXL allow the treatment to be performed on eyes with ultrathin corneas.
It is important to balance hope with realism—particularly when a patient’s situation is at the edge of what is possible or multiple interventions are required. Be frank about the risks and benefits. Explain the decision-making process and, if possible, the scientific evidence underlying your recommendation.
CONCLUSION
The way to win patients for life is to earn their trust. Be open and honest about the pros and cons of every procedure and the likelihood of success. Take the time to explain the science and medicine to them so that they understand the decision-making process and know the advantages and limitations of the options available to them. In short, treat patients how you would like to be treated.
1. Torres Netto EA, Al-Otaibi WM, Hafezi NL, et al. Prevalence of keratoconus in paediatric patients in Riyadh, Saudi Arabia. Br J Ophthalmol. 2018;102(10)1436-1441.
2. Meyer JJ, Gokul A, Vellara HR, McGhee CNJ. Progression of keratoconus in children and adolescents. Br J Ophthalmol. Published online September 3, 2021. doi:10.1136/bjophthalmol-2020-316481
3. Chatzis N, Hafezi F. Progression of keratoconus and efficacy of corneal collagen cross-linking in children and adolescents. J Refract Surg. 2012;28(11):753-758.
4. Gatinel D. Challenging the “no rub, no cone” keratoconus conjecture. Int J Kerat Ect Cor Dis. 2018;7(1):66-81.
5. Hafezi F, Hafezi NL, Pajic B, et al. Assessment of the mechanical forces applied during eye rubbing. BMC Ophthalmol. 2020;20(1):301.
6. Torres-Netto EA, Randleman JB, Hafezi NL, Hafezi F. Late-onset progression of keratoconus after therapy with selective tissue estrogenic activity regulator. J Cataract Refract Surg. 2019;45(1):101-104.
7. Hafezi F. Pregnancy induced changes in corneal biomechanics & topography related to thyroid hormone. Paper presented at: ASCRS Annual Meeting; May 3-9, 2017; Los Angeles, CA.
8. Hafezi F. Tobacco smoking and its impact on corneal biomechanics. Invest Ophthalmol Vis Sci. 2010;51(12):6892.
9. Elsheikh A, Geraghty B, Rama P, Campanelli M, Meek KM. Characterization of age-related variation in corneal biomechanical properties. J R Soc Interface. 2010;7(51):1475-1485.
10. Hafezi F, Koller T, Derhartunian V, Seiler T. Pregnancy may trigger late onset of keratectasia after LASIK. J Refract Surg. 2012;28(4):242-243.
11. Hafezi F, Kling S, Gilardoni F, et al. Individualized corneal cross-linking with riboflavin and UV-A in ultrathin corneas: the sub400 protocol. Am J Ophthalmol. 2021;224:133-142.
12. Hafezi F, Torres-Netto EA, Randleman JB, et al. Corneal cross-linking for keratoglobus using individualized fluence. Journal of Refractive Surgery Case Reports. 2021;1(1).

