




A 61-year-old woman with Graves disease presented to the emergency department with redness and pain in the left eye that had begun 2 days earlier. The patient had undergone traumatic cataract removal in the eye more than 10 years prior.
She reported no recent vision changes but noted that the vision in the left eye had been poor since childhood, unrelated to her history of trauma. The patient had presented to the ophthalmology clinic 9 years prior. A chart review revealed a peripapillary staphyloma and macular scar in the left eye, which was most likely the cause of her chronically poor vision.
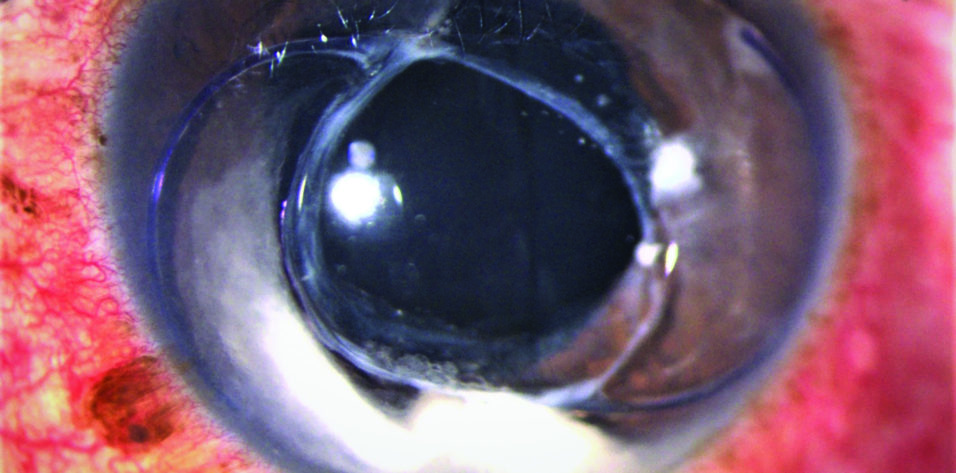
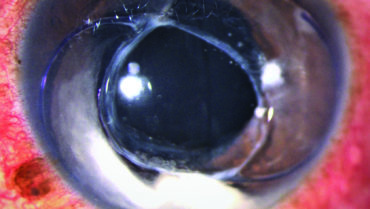
During evaluation in the emergency department, her visual acuity was 20/50 OD and count fingers at 5 feet OS. The IOP was in a normal range in both eyes. An examination found a relative afferent pupillary defect and an abnormal anterior chamber in the left eye. The pupil of the left eye was shaped like a tear drop and appeared larger than the pupil in the right eye.
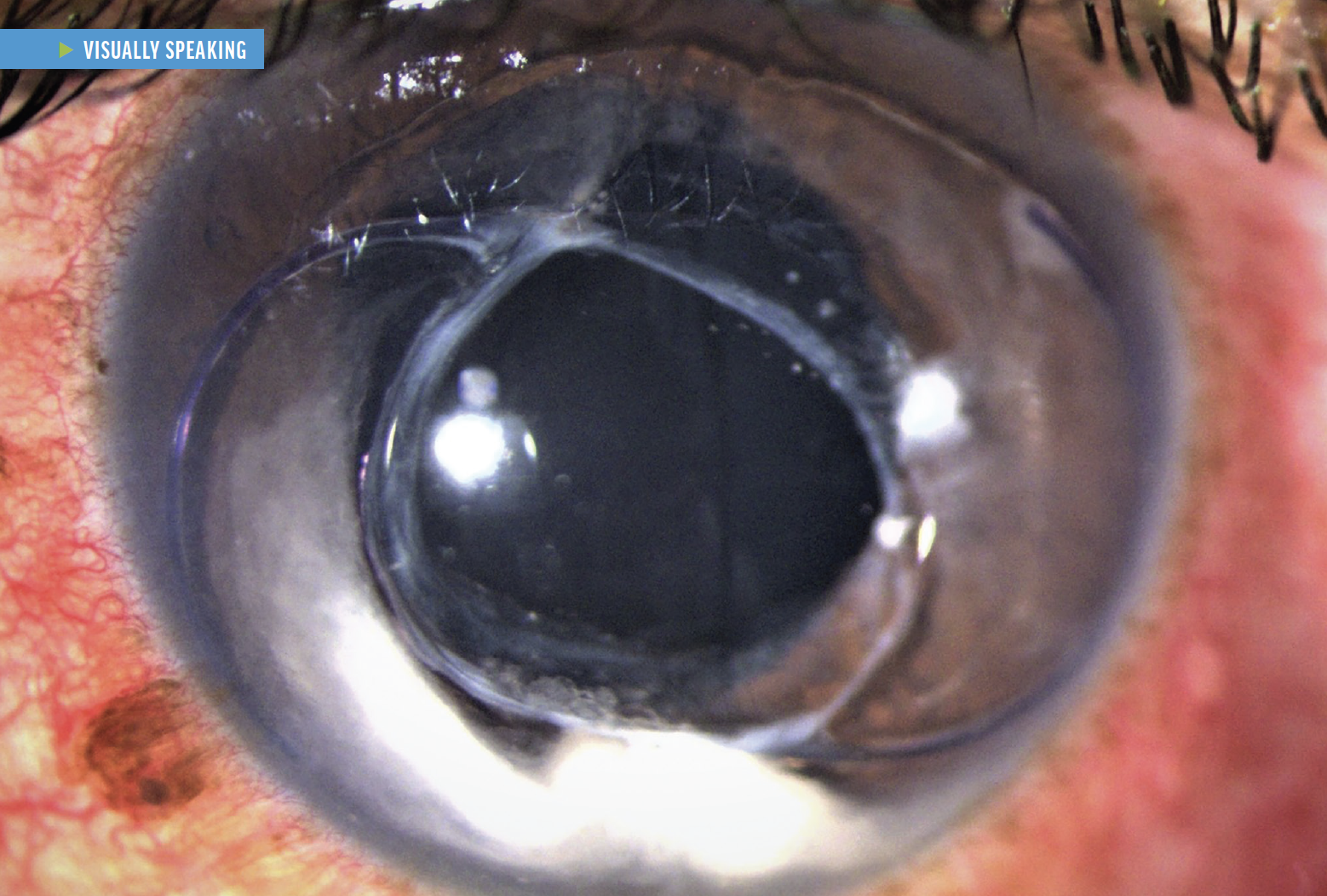
A slit-lamp examination revealed that the entire IOL–capsular bag complex was in the anterior chamber of the left eye. The patient reported no new trauma to the eye and was unsure when the complex had become dislocated. Chart review confirmed that the IOL was originally placed within the bag. With no additional trauma, the dislocation was most likely associated with zonular weakness.
Removal of the IOL–capsular bag complex and placement of a secondary IOL were planned. The patient opted to postpone surgery. She received a prescription for pilocarpine administered three times daily to constrict the pupil and prevent the complex from falling into the vitreous. Despite attempts at contact, the patient was subsequently lost to follow-up.

