



Some of my colleagues consider patients who undergo laser refractive surgery to be one and done. In other words, these individuals come to the clinic, undergo an operation, and leave. Many marketing specialists also share this perspective. I do not.
Many of my patients who undergo laser refractive surgery return to my practice for other personal eye care needs or those of their family members. The key is to become a reliable, long-term partner in patients’ quest for optimal vision.
CHILDREN
First contact. The lifecycle of a refractive surgery patient starts in childhood. Speaking with adult patients who are parents and who are interested in vision correction for themselves presents an opportunity for me to inquire about their children’s vision. I can suggest that their children come in for an examination.
Children may be genetically predisposed to develop astigmatism, for example. The early detection of ocular surface disease and refractive errors can help to maximize their eye health and visual acuity. This can, in turn, improve their academic performance and quality of life.
Children and teenagers. Many youths spend more time viewing screens (eg, computers, tablets, smartphones) than they do playing outside. Poor eyesight may be contributing to the lack of physical activity. The opposite can also be true. Some children benefit from orthokeratology until they reach maturity and their refractive status stabilizes, at which time further decisions on their care can be made. Other patients benefit from contact lenses or spectacles.
LASER VISION CORRECTION
When patients present for a refractive surgery consultation, their long-term plans are a part of the conversation. My recommendations are based on their hobbies, profession, goals, and future plans. For example, a procedure that creates a flap may not be the best option for someone who is keen on sports. Alternatively, a person with low myopia who regularly works at a computer and does not wish to wear spectacles may be an ideal candidate for a flap-based procedure, which can give them the option of future refractive enhancements.
Whatever the plan, I emphasize to patients that professionals such as myself will be available throughout their lives to help them select the optimal solutions for their vision and ocular health. I also stress that it is important for them to retain their preoperative data to share with the treating ophthalmologist if they undergo IOL surgery in the future. Access to this information can improve the accuracy of IOL calculations.
PRESBYOPIA CORRECTION
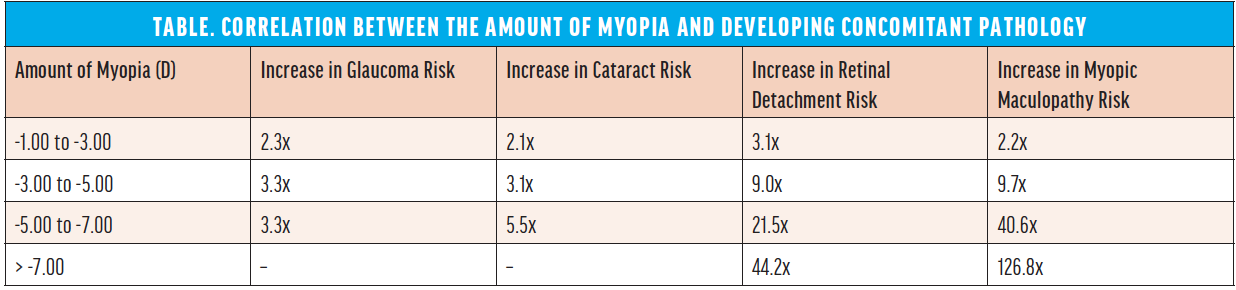
The options for presbyopia correction are expanding. An issue to bear in mind with this patient population, however, is the relationship between myopia and the development of concomitant pathology (Table). I avoid or delay refractive lens exchange for as long as possible, especially in patients with high myopia because of their risk of postoperative complications such as retinal detachment, cystoid macular edema, and IOL decentration.2
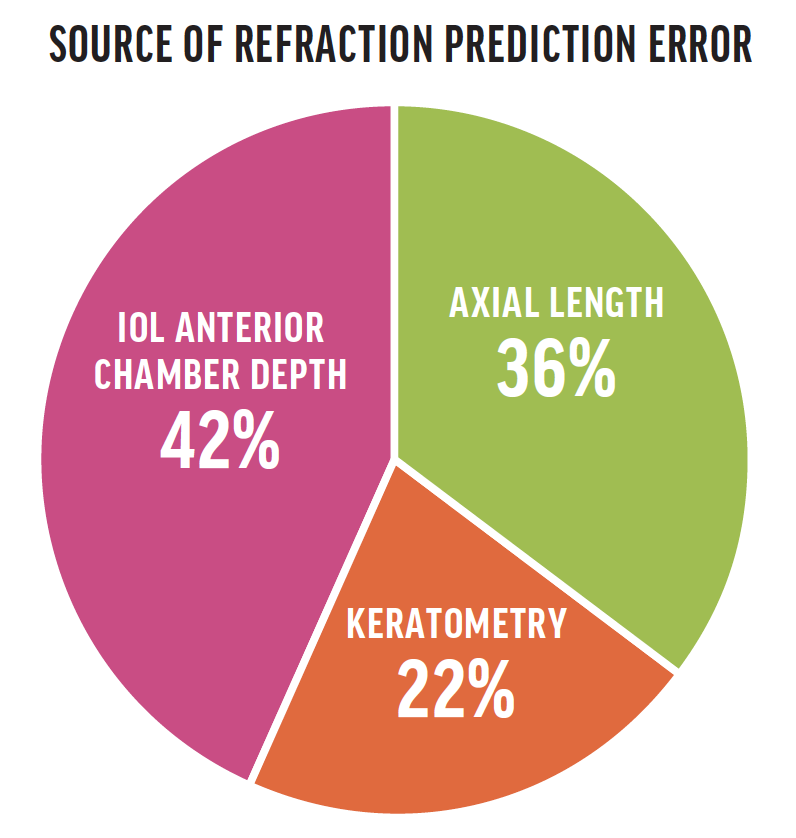
I also explain to these individuals that the accuracy of IOL power calculations is lower in highly myopic eyes (see Source of Refraction Prediction Error).3,4
CONCLUSION
When evaluating young patients for laser vision correction, I bear in mind their future ocular health—presbyopia, cataract, glaucoma, age-related macular degeneration—and discuss it with them as appropriate. The conversation can be challenging, but it also builds our relationship and reinforces the idea that they can return to my clinic for eye care for the rest of their lives.
1. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622-660.
2. Martiano D, Cochener B. Implants multifocaux chez le grand myope, résultats à 6ans. J Fr Ophtalmol. 2014;37(5):393-399.
3. Alió JL, Grzybowski A, Romaniuk D. Refractive lens exchange in modern practice: when and when not to do it? Eye Vis (Lond). 2014;1:10.
4. Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmol Scand. 2007;85(5):472-485.

