Chopping, divide and conquer, and supracapsular are the three primary nuclear disassembly techniques. Louis D. “Skip” Nichamin, MD, is one of the key thought leaders who helped teach and popularize the chopping technique in the late 1990s and early 2000s.
In the early years of my career, I remember watching Skip’s omnipresent video presentations at countless AAO and ASCRS meetings. He and other pioneers of the technique appeared to disassemble nuclei by magic. Chopping remains my primary phaco technique to this day.
Tal Raviv, MD

Discussions of contemporary lens-based surgery often emphasize refractive predictability and visual quality metrics that exceed the limits of traditional Snellen acuity. As remarkable as refinements in these areas have been, a number of simple yet brilliant incremental innovations in phaco technique underscore cataract surgery’s current level of efficiency and safety, particularly for dense nuclei. One of these pivotal developments, known as phaco chop, is an approach to mechanical nuclear disassembly that was designed to take advantage of the lamellar architecture of the crystalline lens (Figure 1). Coupled with the advanced fluidics and power modulation that subsequently became available on phaco machines, the use of this technique improved surgical efficiency, decreased fluid turnover, and minimized cumulative dissipated energy.1

Figure 1. Lens anatomy. Human lens fibers are arranged in lamellae, oriented much like the grain within wood. Reprinted with permission from Moore RL, Silva VDR. The basics of phaco chop techniques. Cataract & Refractive Surgery Today. 2012;12(1):64-66.
INTRODUCTION AND REFINEMENT
In 1993, Kunihiro Nagahara, MD, shocked the ophthalmic community at the ASCRS Annual Meeting in Seattle with his award-winning video demonstrating a means of cataract removal that obviated the need for sculpting and grooving—prerequisites for the divide and conquer technique that was preferred at the time.2 His pioneering approach came to be known as horizontal chop because the chopping instrument was placed peripherally around the equator of the lens before it was drawn centripetally toward the centrally impaled phaco tip (Figure 2A). Variations on the technique quickly emerged.
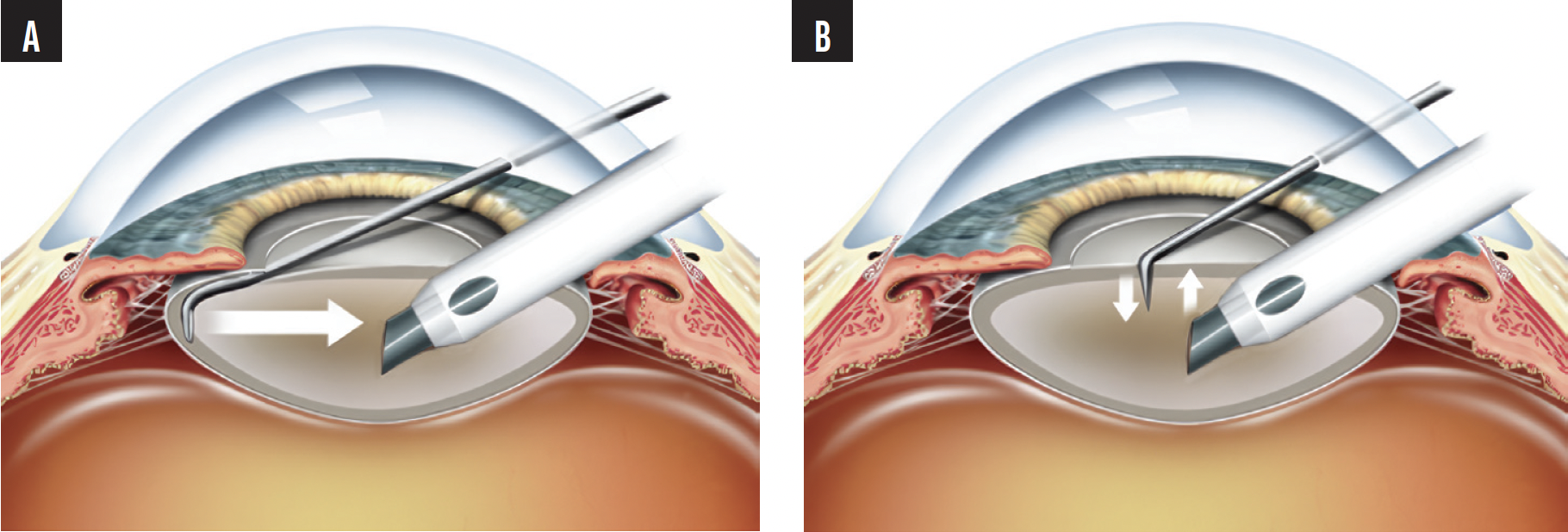
Figure 2. Horizontal (A) and vertical (B) chop. Reprinted with permission from Moore RL, Silva VDR. The basics of phaco chop techniques. Cataract & Refractive Surgery Today. 2012;12(1):64-66.
The stop and chop approach developed by Paul Koch, MD, eased surgeons’ transition from full divide and conquer to a chop technique. With this hybrid modification, an initial groove and nuclear crack were performed to create additional working space, thereby facilitating subsequent chopping.3
Another significant variation known as vertical chop was contemporaneously described by several surgeons, including David Dillman, MD (who coined the term quick chop); Vladimir Pfeifer, MD; Tobias Neuhann, MD; Abhay Vasavada, MD; and Hideharu Fukasaku, MD (known for what he dubbed snap and split).4
HORIZONTAL VERSUS VERTICAL CHOP
Fundamentally, what distinguishes vertical from horizontal chop is more central placement of the chopping instrument, just in front of or beside the impaled phaco tip (Figure 2B). With the sideport incision used as a fulcrum, the manipulator is moved in a downward motion (Figure 3A). After the initial vertical vector force between the manipulator and the stabilizing phaco tip is established, horizontal displacement of the instruments may be required to complete the cleavage plane through the posterior nuclear plate, especially for nuclei of greater density (Figure 3B). For extremely dense lenses, preliminary sculpting and central debulking may be helpful to decrease the force required during the initial chop.

Figure 3. Vertical chop initiated after deeply impaling the nucleus with a phaco needle (A). After vertical motion, instruments are separated laterally, propagating division (B). From: Phaco Chop and Advanced Phaco Techniques. Chang D, ed. 2nd ed. © 2013 by Slack. Reproduced by permission of Taylor & Francis Group.
In practice, many surgeons employ both horizontal and vertical chop techniques and base the decision of which to use on the cataract and other ocular characteristics. I often used both techniques during a single case; I would begin with vertical chop and transition to horizontal subsectioning, thereby creating bite-sized segments that could be aspirated more easily.
Prechop, as originally described by Takayuki Akahoshi, MD, is another viable option, particularly for lenses of modest density. The mechanical separation of nuclear segments is achieved before the phaco instrument’s insertion. This can be accomplished with a specialized unimanual instrument or bimanually with two separate manipulators.
RECEPTION AND ADOPTION
The transition from extracapsular cataract extraction to phacoemulsification required a huge shift in surgeons’ mindset and a great deal of education and training. The transition from divide and conquer to phaco chop, in contrast, was more of an incremental change.
When phaco chop and the first variations on it were introduced, surgeons were motivated to learn the technique because its efficiency was immediately apparent; sculpting and grooving decreased, and significantly less phaco energy was required. A hush fell across audiences as they first watched Dr. Nagahara’s demonstrations. In short, phaco chop had a “wow” factor.
For most surgeons, the greatest obstacle to learning phaco chop was that the technique demanded increased bimanual dexterity—something not heretofore required for nuclear disassembly. During divide and conquer, the nondominant hand is used only briefly, after creation of the groove, to separate the nuclear halves and subsequent quadrants.
Another hurdle was that horizontal chop requires passage of the chopping instrument out to the periphery, underneath the anterior capsule, around the cataract, and then toward the phaco instrument. This maneuver was scary as the chopping instrument came into close proximity with the capsule and part of the excursion had to be completed without full visualization.
Success with horizontal chop, therefore, required surgeons to become more dexterous with their nondominant hand and practice using their hands together, to become cognizant of where each instrument was in the eye, and to muster the confidence to venture into peripheral areas that were close to the lens capsule.
INSTRUMENTATION
Early phaco chop was often performed with whatever manipulator or hook the surgeon had on hand, typically a Sinskey hook. The instruments were too short to reach around the equator of the lens, engage the material, and create a separation plane effectively.
These limitations inspired me to design my first chopper. The instrument was longer than the available manipulators and hooks at the time, and it had a beveled inner edge that could penetrate the lens material more efficiently. The tip was blunt to avoid snagging the capsular bag, and it was substantial enough to mechanically divide and separate the nuclear segments.
The shift from horizontal to vertical chop led to more new instrument designs (Figure 4). Compared to the first choppers, the next wave of instruments had a sharper, beveled, thin, or flattened tip to facilitate penetration into the lens.

Figure 4. This instrument was designed by Dr. Nichamin for vertical chop and was one of his favorites. It was originally manufactured by Storz/Bausch + Lomb.
With both horizontal and vertical chop, the impaled phaco tip fixates the lens, providing countertraction to the chopper.
TECHNICAL AND TECHNOLOGICAL ADVANCES
Surgeons’ adoption of the phaco chop technique spurred improvements in phaco technology. The removal of mechanically chopped nuclear segments required different phaco power dynamics and fluidics. The sculpting and grooving required in divide and conquer demanded lower flow rates, lower vacuum levels, and higher, often continuous power. Industry responded to the development of phaco chop by creating new and refined energy modes such as pulsed and burst. This, combined with optimization of the phaco needle design and a more retracted sleeve position, promoted the deep, secure purchase of nuclear segments.
As with any endocapsular technique, thorough hydrodissection was employed to minimize stress on the lens capsule and zonules during rotational maneuvers. Many surgeons would also perform hydrodelineation to create a smaller endonuclear mass that was easier to chop. The delineation of an outer epinucleus, meanwhile, helped protect the capsule during nuclear disassembly. Lastly, properly sized and crafted incisions and precise fluidics settings helped stabilize the anterior chamber.
CONCLUSION
Phaco chop and its various iterations offer surgeons an efficient means by which to leverage the inherent cleavage planes within the human crystalline lens. Although the technique requires a degree of bimanual dexterity, it can significantly enhance the ease and safety of cataract removal, particularly for lenses of greater density.
1. Fernández-Muñoz E, Chávez-Romero Y, Rivero-Gómez R, Aridjis R, Gonzalez-Salinas R. Cumulative dissipated energy (CDE) in three phaco-fragmentation techniques for dense cataract removal. Clin Ophthalmol. 2023;17:2405-2412.
2. Nagahara K. Phaco chop. Film presented at: International Congress on Cataract, IOL and Refractive Surgery, ASCRS; May 1993; Seattle, WA.
3. Koch PS, Katzen LE. Stop and chop phacoemulsification. J Cataract Refract Surg. 1994;20(5):566-570.
4. Nichamin LD. Vertical chopping principles and pearls. In: Chang DF, ed. Phaco Chop and Advanced Phaco Techniques: Strategies for Complicated Cataracts. 2nd ed. Slack; 2013:21-24.