
During lab development and several weeks of pre-market use, I had the opportunity to try the CENTURION Vision System’s (Alcon) new ACTIVE SENTRY Handpiece (Alcon) in various clinical situations and determine whether it makes a positive difference in surgery. During cataract surgery, sensors incorporated in the ACTIVE SENTRY Handpiece continually communicate with the system’s ACTIVE FLUIDICS (Alcon) component, which in turn makes instant, automatic adjustments to maintain a stable anterior chamber. In using this technology, I found that the ACTIVE SENTRY made a marked difference in chamber stability throughout my cataract procedures. In fact, the improvement was so pronounced that I didn’t want to return to the standard handpiece.
Responsive Handpiece Sensor
When the pressure sensor is located in the fluidics module, the pressure change must be transferred through the collapsible tubing. It’s a delay of many milliseconds, and by the time the system senses a change, it may be too late to respond to the surge. This results in some fluctuation in the chamber that can be problematic or cause complications, particularly if the surgeon is working at a higher vacuum and/or flow rate. By moving the sensor to the ACTIVE SENTRY Handpiece, the delay is minimized, and the system can correct drops in pressure more quickly and better control any surge.
This invaluable function is transparent to the surgeon, who does nothing differently and hears no indication that correction has occurred. In many cases, after finishing a case, I did not know if the ACTIVE SENTRY had triggered surge protection at all. When I looked at the metrics, I found it had activated 15 to 20 times in the background, automatically helping to prevent fluctuation of the chamber without distracting me.
When the ACTIVE SENTRY senses a sudden drop in IOP, as we would see with an occlusion break, the CENTURION ACTIVE FLUIDICS very quickly mitigates the change in pressure.
The primary benefit of the ACTIVE SENTRY Handpiece is to improve chamber stability, which means better safety. If your chamber is not volatile, your procedure is safer. Efficiency is a secondary benefit. Without an automated system, we can do one of two things when we detect volatility: change our settings or work more slowly. Automation eliminates those inefficiencies.
Appropriate for Most Cases
During the weeks that I had the ACTIVE SENTRY in our surgery center, I used it for all types of cases. The handpiece provides benefits, regardless of what we think preoperatively about the likelihood that the patient will have volatile chambers. In reality, volatility is very hard to predict. We know it’s likely in certain patients, such as overweight patients with significant orbital fat, patients with tight lids, and high myopes. But even in apparently routine cases, some volatility can occur.
In addition to maintaining a stable chamber during surgery, the ACTIVE SENTRY helps to eliminate one common reason for chamber volatility in otherwise normal cases: inaccurate eye level settings. The ACTIVE SENTRY Handpiece automatically detects the patient’s eye level. Without this feature, the surgeon or scrub technician needs to set the eye level manually to ensure that we’re operating at the desired pressure. I believe that many surgeons may sometimes not take the time to set the level manually, and the result may be increased chamber fluctuation. Like pressure sensing in the ACTIVE SENTRY, automated eye level setting ensures a more stable chamber and safer surgery.
With this reliable stability and added safety comes surgical confidence. With the ACTIVE SENTRY, we learn to perform procedures without worrying about volatility in the chamber. It’s another benefit that’s valuable in every case.
The ACTIVE SENTRY is designed with the comfortable ergonomics required to bring instruments into everyday surgical use. The handpiece is at least as comfortable as the current alternative and approximately 10 g lighter. I could use it all day without discomfort or fatigue.
Added Safety: INTREPID Hybrid Tip
The polymer I/A tip (Alcon) was surgeons’ first introduction to polymer tips, and it quickly gained a groundswell of support. Many surgeons have moved to the polymer I/A tip because it helps to boost safety. To me, it’s an example of the best kind of tool—one that can improve outcomes and makes us better surgeons by enhancing safety and efficiency.
The next step in polymer instruments for cataract surgery is the CENTURION Vision System new INTREPID Hybrid Tip (Alcon). Despite my affinity for the polymer I/A tip, I approached the Hybrid Tip with my usual skepticism, asking if and how it would benefit my procedures. I wondered how a polymer tip could be as efficient as a standard tip without having any sharp metal edges.
When I tried the Hybrid Tip, I found that it cuts very well and does not have any negative effect on my efficiency. More importantly, the Hybrid Tip is much less likely to break or damage the capsule if we inadvertently make contact. Any metal tip can have a little burr, scratch, or chip on an edge, which can catch on the capsular bag. That can’t happen with a single-use, disposable polymer Hybrid Tip. It’s soft and kind to whatever tissue it engages.
At the same time, the Hybrid Tip can remove segments of the nucleus and make grooves for a divide-and-conquer approach, even in a grade 3 cataract. Like a metal tip, as soon as the Hybrid Tip gets a piece of the nucleus inside it, it creates vacuum to remove the segments. The only case where you may lose some efficiency in low vacuum sculpting is with a mature or brunescent cataract, yet it still can perform well once the cataract is fragmented.
Combined Advantages
I believe that once surgeons try the ACTIVE SENTRY Handpiece, they’re going to want to use it in every case. The combination of the ACTIVE SENTRY and the Hybrid Tip will be very powerful in improving safety and efficiency. Relying on their combined advantages during surgery, my confidence that I would perform a case without any major complication went way up. I could work more efficiently and increase my vacuum levels, knowing with confidence that the procedure would be consistent and controlled.
Case: Floppy Iris and Zonular Weakness
My patient had a grade 2 nuclear sclerotic cataract and underwent cataract surgery with placement of a toric IOL. The patient also had a floppy iris due to using tamsulosin (Flomax; Sanofi). I used the ACTIVE SENTRY Handpiece with its built-in pressure sensor, which works closer to the action to detect changes in pressure and initiate a response more quickly, compared to using a sensor placed further back in the fluidics system.
Floppy iris and zonular weakness: Because the patient had a small pupil and floppy iris, I decided to place a Malyugin Ring (MicroSurgical Technology). During the capsulotomy, I determined that the bag felt a bit floppy as well; I suspected there could be some zonular weakness.
I didn’t want to displace the entire nucleus, which could damage zonular fibers that were already weak. After hydrodissection with a Chang Cannula (Katena), I used a two-handed rotation method to free the nucleus and avoid displacing it, which could damage the zonular apparatus. Next, I tried to pre-chop. I was able to get a little bit of divide, but visualization was not great; I proceeded with phaco to avoid zonular damage.
Phacoemulsification with the Hybrid Tip: The ACTIVE SENTRY Handpiece maintained a nice, stable chamber, even with a floppy iris and some weakened zonular fibers. Using the polymer Hybrid Tip, I carefully divided the nucleus (Figure 1). As I segmented each quadrant, the ACTIVE SENTRY vacuum removed it quickly and efficiently while maintaining a rock-solid, stable chamber. The lens was a little resistant to rotation, so instead of challenging the zonular fibers, I used the two-handed method to encourage it to turn.
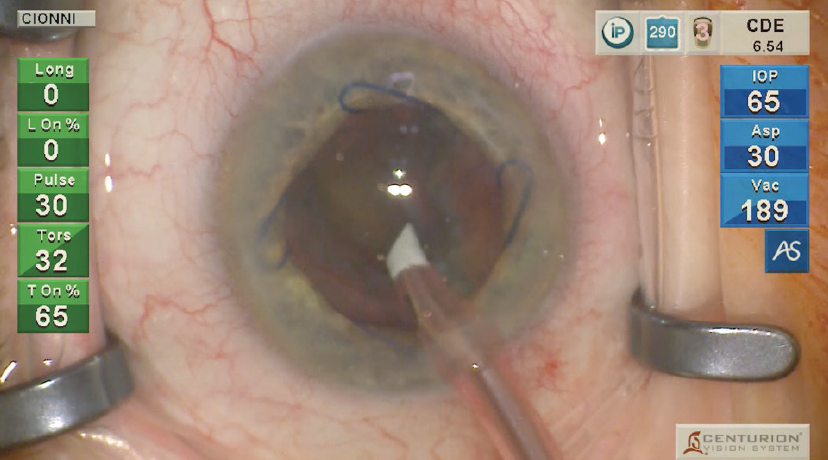
Figure 1. This patient had a floppy iris and zonular weakness. The rounded polymer INTREPID Hybrid Tip allowed me to divide the nucleus of this grade 2 cataract and vacuum away each quadrant quickly and efficiently, while the ACTIVE SENTRY Handpiece maintained a rock-solid, stable chamber.
Once pieces began coming into the tip, I could keep the tip still. The followability was so good with the fluidics that segments moved into the tip. Again, the chamber remained stable. Occasionally during quadrant removal, I could see a blue flashing light on the monitor, indicating that ACTIVE SENTRY was reacting to a sudden drop in pressure and opening the vent to allow more fluid to come into the line and mitigate the occlusion break surge. Finally, I flushed all the angles with BSS (Alcon) to make sure no nuclear chips remained.
Cortex removal and polishing: Next, I began cortex removal with the polymer I/A tip (Figure 2). The polymer construction is much less likely to damage the capsule than a sharp metal tip, and the tip is disposable, so we don’t have to worry about defects that could come from cleaning it. We use a brand new one every time.
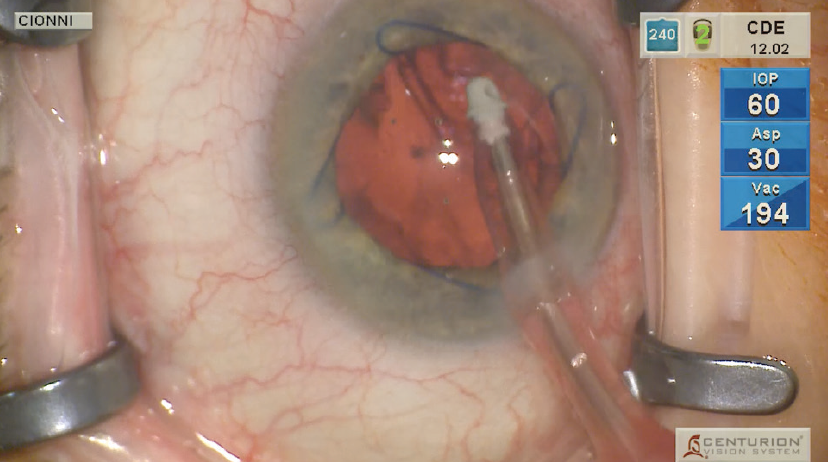
Figure 2. Cortex aspiration with the polymer I/A tip reduced the likelihood of capsular damage. As I used the polymer I/A tip to remove the cortex and polish the floppy capsule, I could barely generate any vacuum. It would just collapse. This weakness showed just how well the ACTIVE SENTRY had excelled at maintaining a stable chamber during phacoemulsification.
As I polished the floppy capsule, I could barely generate any vacuum before it would wrinkle. It was a real testimony to how the ACTIVE SENTRY had kept a very floppy iris and floppy bag stable throughout phacoemulsification. In addition, the added level of safety afforded by the polymer I/A tip helped ensure that there was no rupture when the capsule did come forward.
Implanting the toric lens: To place the IOL, I filled the bag with sodium hyaluronate (PROVISC; Alcon) OVD and gently injected the lens in the bag. Going behind the implant with the polymer I/A tip, I removed the viscoelastic, centered the implant, and aspirated into the angles. Finally, I hydrated the incision. What could have been a very challenging case was made easier by the ACTIVE SENTRY, as well as the Hybrid Tip and polymer I/A tip.



