


CASE PRESENTATION
A 64-year-old woman presents for a cataract evaluation. The patient underwent radial keratotomy (RK) outside the United States many years ago—six RK incisions in the right eye and eight RK incisions plus two astigmatic keratotomy incisions in the left eye. She also underwent retinal detachment (RD) repair by scleral buckle and cryotherapy in the right eye 10 years ago. She has a known history of hypothyroidism without thyroid eye disease and superior limbic keratoconjunctivitis that is being managed by another doctor with sodium chloride hypertonicity ophthalmic ointment 5% (Muro 128, Bausch + Lomb) at bedtime.
The patient has experienced blurry vision, glare, and halos—all to a much greater degree in the left versus right eye—for 2 years. She reports previously having good vision and says that it does not fluctuate during the day. She works as a caregiver at a preschool and enjoys gardening, swimming, hiking, and walking her dog.
On examination, the patient’s UCVA is 20/40+2 and J5-2 OD and 20/400, 20/50 with pinhole testing, and J3 to J2 OS. Her BSCVA is 20/25-2 with a refraction of +0.50 -2.00 x 11º OD and 20/40-1 with a refraction of -4.50 -2.00 x 169º OS. Ocular dominance testing reveals a dominant right eye.
At the slit lamp, superior corneal staining and a 1+ nuclear and cortical cataract are evident in the right eye. The RK incisions in that eye are relatively straight and symmetrical but located close to the visual axis. No gaping or epithelial plugging of the incisions is observed. The appearance of the left eye is similar. In addition to superior corneal staining, 3+ dense nuclear sclerosis and 1+ cortical changes are observed in that eye.
A fundus examination reveals a blunted reflex, an epiretinal membrane, and a lamellar macular hole in the right eye. The findings are confirmed with OCT (Figures 1–3). A scleral buckle, peripheral chorioretinal atrophy, and scarring are also evident. Superior laser retinopexy scars are observed in the left eye, but the fundus is otherwise healthy.

Figure 1. Analysis of the right (A) and left (B) eyes with the OPD Scan (Nidek).
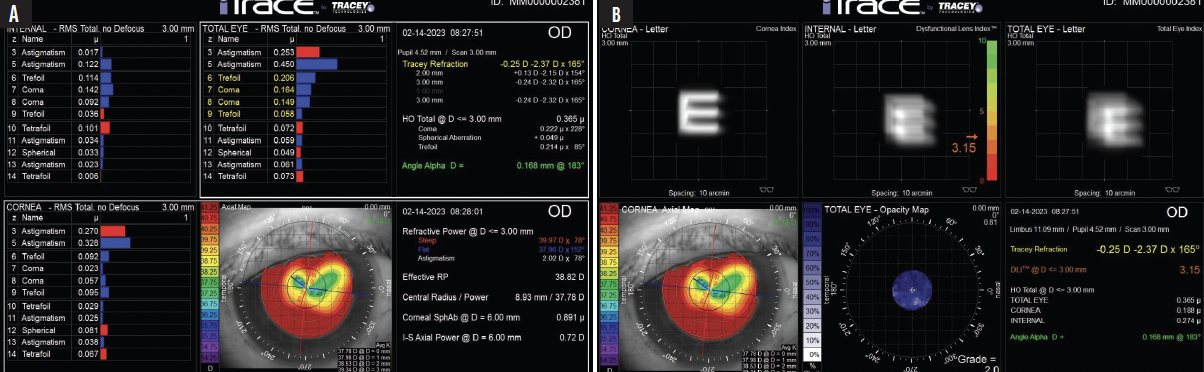
Figure 2. Aberrometry measurements with the iTrace (Tracey Technologies), root mean square (A) and total eye (B), of the right eye.

Figure 3. iTrace aberrometry measurements, root mean square (A) and total eye (B), of the left eye.
The patient wishes to reduce her dependence on glasses and contact lenses. She has no interest in wearing rigid gas permeable (RGP) lenses. She does not recall if she has experience with monovision or if the visual acuity of her eyes was similar before she developed cataracts. She says the vision in her right eye was never the same after the RD.
What are the chief considerations in this case? Which IOL would you recommend, and what would your second choice of lens be? For the purposes of discussion, assume that your options include a Light Adjustable Lens (LAL; RxSight) and IC-8 Apthera (Bausch + Lomb). If an LAL is your first choice and the patient is dissatisfied with her vision after surgery due to poor BCVA, would you exchange the LAL for an Apthera or a monofocal lens? Would you charge her for the exchange and new IOL? If an Apthera is your first choice and it must be exchanged for power or patient dissatisfaction with dimming of vision, would you exchange the lens for an LAL or a monofocal IOL? When do you perform an RGP contact lens overrefraction in patients who have a history of RK—before or after cataract surgery? Do you have an aberrometry or BSCVA cutoff for moving from an LAL to an Apthera lens?
— Case prepared by Neda Nikpoor, MD

VANCE THOMPSON, MD
First, I want to understand the sources of blur. An RGP contact lens overrefraction is a must before any decisions are made. If the patient’s BSCVA improves from 20/25-2 to 20/20-2 OD and from 20/40-1 to 20/25 OS, the corneas are responsible for 1 and 2 lines of blur in the right and left eyes, respectively.
When the cornea is a significant source of blur in a patient with cataracts, only the IC-8 Apthera can improve both, but it would not be my first choice here. The post-RK corneal topography is well centered, the incisions are well healed with no epithelial plugging, and the patient was happy with her postoperative vision for many years. All of this suggests that the procedure was a success and she took good care of her eyes by not rubbing them. I therefore suspect that an RGP contact lens overrefraction may improve her vision slightly but not enough to change my thinking that an LAL would give her the best chance of minimizing her refractive error. Given the patient’s history of corneal surgery, hypothyroidism, and superior limbic keratoconjunctivitis, I want to touch her cornea as little as possible. The LAL’s adjustable optic is therefore preferable to an IOL for which addressing residual refractive error would entail corneal surgery. My second choice, which I used in situations like this one before the LAL became available, would be a monofocal IOL. I would explain to the patient why wearing glasses to correct her residual refractive error is reasonable.
If the patient is dissatisfied with her UCVA and BCVA after surgery with the LAL, the RGP contact lens overrefraction would be repeated. Based on preoperative findings, I do not believe the overrefraction would produce a significant improvement. The extended depth of focus inherent in the LAL is not known to reduce image quality. The patient would therefore most likely be encouraged to allow time for neural adaptation to occur and counseled that the retina influences image quality, so the risks entailed by an IOL exchange are not worth taking. An IOL exchange is included in the price of our premium package, but the procedure is rarely required.
I do not have an aberrometry or BSCVA cutoff for moving from an LAL to an IC-8 lens. I value the aberrometry measurement, but it is a significant improvement in BSCVA with an RGP contact lens overrefraction that prompts me to recommend the IC-8 instead of the LAL to patients who have irregular corneas.
I participated in the FDA-monitored trials of the LAL and IC-8 and am a big fan of both technologies in the right situations. I typically implant the IC-8 in the nondominant eye. The patient in this case reported that the vision in her right eye was never the same after RD repair. I do not want to reduce contrast sensitivity in her better-seeing, nondominant left eye.

ROGER ZALDIVAR, MD, MBA
Several details about the patient’s right eye make me leery of implanting a small-aperture IOL. First is the RD repair by scleral buckle and cryotherapy 10 years ago. Second and third are the epiretinal membrane and lamellar macular hole. To preserve contrast sensitivity, I would choose a monofocal IOL or, theoretically, an LAL. I use the word theoretically because I do not have experience with the LAL but appreciate the technology’s ability to overcome difficulties in IOL power calculation through postoperative adjustment. Thanks to advances in IOL formulas for post-RK eyes, I no longer perform RGP contact lens overrefractions before or after cataract surgery on patients who have a history of RK.
My approach to the left eye would be different because it has eight RK cuts and a healthy retina. My first choice of IOL would be an IC-8 Apthera. The low magnitude (0.25 µm) of corneal higher-order aberrations (HOAs) notwithstanding, implanting an IC-8 lens could improve the patient’s optical quality at night by neutralizing the effects of the RK incisions and extend depth of focus for daily activities.
My decision to move from a monofocal to an IC-8 lens is based on aberrometry measurements. My cutoff for the transition is around 0.5 µm of corneal HOAs in healthy eyes. My refractive target is -0.75 D in a nondominant eye. If both of a patient’s eyes have a high magnitude of corneal HOAs, bilateral implantation of an IC-8 lens may be considered.

WHAT I DID: NEDA NIKPOOR, MD
As Drs. Thompson and Zaldivar discuss beautifully, several factors must be considered when choosing an IOL. For a patient who has a history of RD, there is a tug-of-war between a desire to reduce aberrations with a small-aperture IOL and avoid a decrease in contrast sensitivity. Some surgeons, moreover, would worry about placing a silicone IOL in this situation. I am less concerned about that because a skilled retina surgeon can often repair a recurrent detachment without oil and, in the event of an IOL opacity, exchange the lens if necessary.
Given the patient’s good visual acuity before cataract formation and reasonable aberrometry measurements, she was likely to see well with a monofocal lens. The LAL is my monofocal IOL of choice for individuals who have a history of refractive surgery, particularly RK. I find its adjustability invaluable in this situation.
Dr. Zaldivar reasonably states that an IC-8 Apthera could be placed safely in the left eye. That said, the patient’s history of an RD and maculopathy in the right eye and retinal tears in the left eye disinclined me toward a small-aperture IOL. After a long discussion, she preferred to avoid the possible reduction in contrast sensitivity and other potential issues if an RD develops in the left eye in the future. She also wished to maintain the best possible quality of vision in her better-seeing eye. We decided to implant an LAL with the understanding that, if her vision did not improve satisfactorily and a subsequent RGP contact lens overrefraction revealed the cornea to be the culprit, the LAL could be exchanged for an IC-8 lens.
Surgery on the left eye was performed a few weeks before this writing. The patient’s BCVA is 20/30+ OS with a refraction of +1.50 -2.00 x 130º. Once the refraction stabilizes, the first light adjustment to the LAL will be performed, and surgery on the right eye will be performed. An LAL is also the first choice for her right eye.

