



Cataract surgeons regularly encounter eyes with weak zonules. The frequency of these encounters will increase because of the aging population and the relative shortage of ophthalmic surgeons.1 Fortunately, advances in surgical technique and instrumentation continue to expand the repertoire of tools that you can use to achieve successful outcomes.
PREOPERATIVE WORKUP
History. Start by obtaining a thorough history. Do not be afraid to repeat questions that your technician might have asked or that were listed in the screening paperwork. Inquire if the patient has experienced ocular trauma and, if so, ask about its nature. Even mild to moderate blunt trauma can alter the zonular apparatus and predispose an eye to zonular weakness intraoperatively. Has the patient seen well out of each eye since childhood? Is there a history of amblyopia? Is there a history of ocular surgery? Prior eye surgery, particularly a pars plana vitrectomy, a glaucoma filtering procedure such as a trabeculectomy, or intravitreal injections can directly or indirectly damage the zonules. Does the patient have systemic medical problems such as Marfan syndrome, Ehlers-Danlos syndrome, homocystinuria, or Weill-Marchesani syndrome? These all affect the connective tissues of the body and can weaken the zonules.2
Examination. Pay close attention to the manifest and/or cycloplegic refraction. Patients with high myopia or hyperopia can have weak zonules. Perform a thorough and detailed slit-lamp examination. Closely examine the pupils. Poor dilation may correlate to zonulopathy or be a sign of pseudoexfoliation syndrome.3 Examine the anterior lens surface for pseudoexfoliative material. With the patient looking straight ahead, gently bump the base of the slit lamp to evaluate the lens for phacodonesis. If one eye has already undergone cataract surgery, examine the IOL for phacodonesis. A visible edge of the lens equator with normal to subnormal pupillary dilation may indicate severe zonulopathy. Further, it may herald the presence of a connective tissue disease such those listed earlier. A dilated funduscopic examination is useful for assessing the edge of the lens for gaps in the zonules and looking for vitreous that might have prolapsed anteriorly. It can also be useful to make sure that no silicone oil or gas is present if the patient had prior retinal surgery.
RECOGNIZING DIFFERENCES
Each patient’s tissues are different. Zonular issues may be more straightforward in young patients compared to elderly patients or those with a history of multiple eye surgeries. For instance, I recently operated on a 33-year-old woman with a history of trauma to her left eye from an airbag injury 15 years earlier. The preoperative examination showed posterior synechiae and a fibrosed and wrinkled anterior capsule, inadequate pupillary dilation, and a 3+ anterior subcapsular cataract. During surgery (scan the QR code now to watch the procedure), the anterior capsule wrinkled when I attempted to puncture it with capsulorhexis forceps (Figure 1A). This confirmed my suspicion that the zonules were weak. I switched to a cystotome needle to open the anterior capsule before completing it with Utrata forceps (Figure 1B).
Once the capsulorhexis was complete, a capsular hook was placed temporally to stabilize the capsule during phacoemulsification (Figure 1C). The lens was soft, likely owing to the patient’s age, and was easily removed. A capsular tension ring was placed before cortical removal to stabilize the capsular bag (Figure 1D). A one-piece monofocal IOL was inserted, and the case was completed without complication.
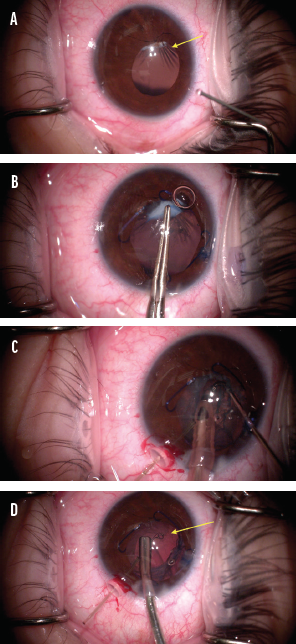
Figure 1. The arrow designates the wrinkled anterior capsule (A). The capsulorhexis is performed with Utrata forceps (B). Phacoemulsification is performed with a capsular hook in place (C). A capsular tension ring inserted (D).
I believe that, despite the prior trauma, the youthfulness of the intraocular tissues contributed positively to the surgical outcome. Had the patient been older or had the zonules been more unstable, the use of a capsular tension segment might have been indicated.
A BIGGER TOOLBOX
Working at a large referral practice, I handle complex anterior segment cases from other ophthalmologists in the region. Zonular issues, sometimes after the cataract procedure, are often encountered. Based on my experience, I recommend expanding your toolbox of surgical techniques to deliver a successful outcome to each patient. Having alternatives can salvage a case, as the following two examples demonstrate.
Case example No. 1. A 56-year-old woman underwent cataract extraction and IOL placement without a rupture of the posterior capsule, but the referring surgeon intraoperatively observed zonular weakness. During the postoperative period, displacement of the IOL–capsular bag complex and a focal iris transillumination defect were observed, and the patient developed cystoid macular edema (CME). Because the IOL–capsular bag complex was unstable and causing anterior chamber inflammation and CME, after obtaining informed consent, I performed an IOL exchange and an anterior vitrectomy (Figure 2; scan the QR code now to watch the procedure).
Initially, I attempted simply to explant the one-piece IOL from the capsular bag, but I noted a large inferior zonular dialysis (Figure 2A). For this reason, the IOL–capsular bag complex was dialed to a position anterior to the iris with a Sinskey hook (Figure 2B). The entire IOL–capsular bag complex was removed, and a thorough anterior vitrectomy was performed (Figure 2C). An anterior chamber maintainer was placed, and a CT Lucia 602 three-piece IOL (Carl Zeiss Meditec) was fixated to the sclera using the Yamane technique4 without complication (Figure 2D–F). To prevent the IOL from interacting with the iris, a peripheral iridectomy was made with the vitrectomy cutter (Figure 2G). The patient did well postoperatively. Visual acuity improved, and the CME resolved almost completely (Figure 2H and I).
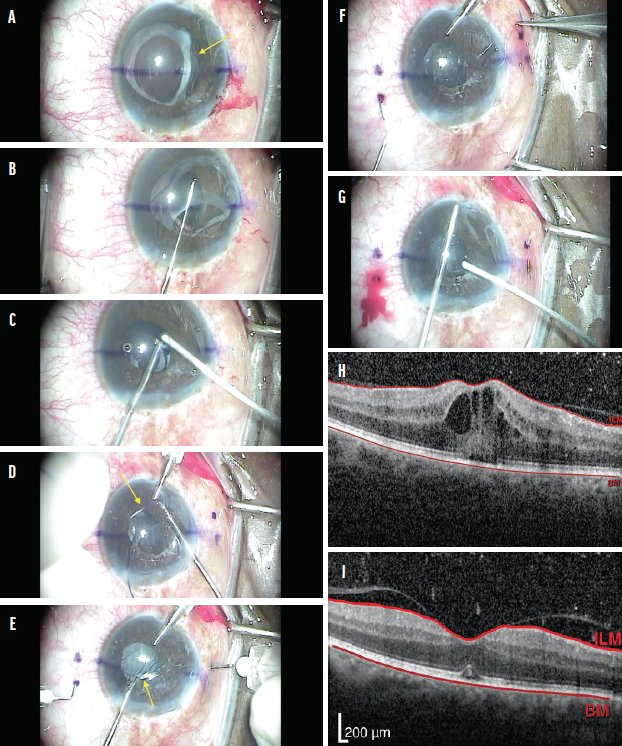
Figure 2. The IOL–capsular bag complex is loose due to inferior zonular loss (A). The complex is removed with a Sinskey hook (B). An anterior vitrectomy is performed, and the capsular bag is removed (C). The leading haptic (D) and then the trailing haptic (E) are passed into a TSK needle. Both haptics are externalized successfully (F). A peripheral iridectomy is created (G). Preoperative macular OCT shows CME (H), and postoperative macular OCT shows its resolution (I).
Case example No. 2. A patient in her 80s was referred for an evaluation of severe zonular weakness after cataract surgery on her second eye. During surgery on the first eye, the referring ophthalmologist noticed mild zonular weakness but placed an IOL without incident. During surgery on the second eye, the cataract was removed without complication, but a large temporal zonular dialysis occurred after the IOL was implanted in the capsular bag.
I saw the patient 2 days after surgery. Upon examination, the pupil was dilated, the IOL–capsular bag complex had decentered nasally, and a 3– to 4–clock hour area of zonular loss had been replaced with vitreous. I determined that the IOL–capsular bag complex was unstable and required removal and suggested that the IOL be exchanged for an anterior chamber IOL.
After a discussion of the risks and benefits of, the alternatives to, and the indications for surgery, the patient chose to proceed with an IOL exchange. During surgery, it was noted that the IOL–capsular bag complex was extremely loose inside the eye and the remaining zonular attachments were weak. The IOL–capsular bag complex came out easily, and a thorough anterior vitrectomy was performed. After the instillation of acetylcholine (Miochol-E, Bausch + Lomb) into the anterior chamber, the pupil was minimally responsive, so I deferred my initial plan to implant an anterior chamber IOL.
One month later, after the eye had healed from the first surgery, IOL calculations and corneal topography were repeated. I recommended the placement of a secondary IOL and a pupilloplasty. After a thorough discussion, the patient chose to proceed. First, the Yamane technique4 was used to sclerally fixate a CT Lucia 602 IOL, which occurred without complication. I feared leaving the pupil fixed and dilated would lead to glare and light sensitivity. Therefore, next, a four-throw pupilloplasty5 using a 10-0 polypropylene suture on a CIF needle (Prolene, Ethicon) was performed at the superior and inferior parts of the pupil to reduce its size. A small opening was purposely left in the superior iris to create a peripheral iridectomy (Figure 3).
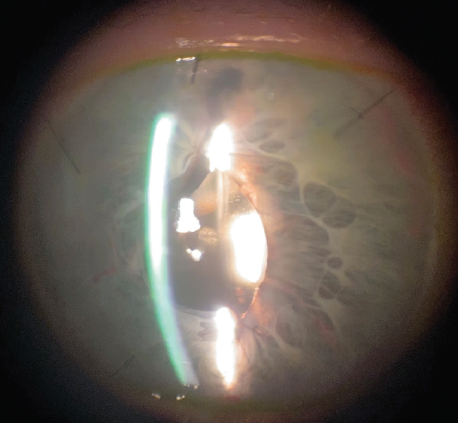
Figure 3. A slit-lamp photograph taken after an IOL exchange using the Yamane technique and a four-throw pupilloplasty.
Postoperatively, BCVA was 20/40, and the patient has done well.
CONCLUSION
I recommend taking a thorough history from each patient who sees you for a surgical consultation. A detailed preoperative examination can identify common and uncommon causes of zonular weakness. Also keep in mind that the age and condition of a patient’s ocular tissues make each surgery unique.
In an era of rapidly evolving anterior segment surgical techniques, having as many tools in your toolbox as possible is helpful. Knowing how to perform an IOL exchange in the setting of weak zonules and mastering several iris repair techniques can be deciding factors in the success of cataract surgery.
1. Ascaso FJ, Huerva V, Grzybowski A. Epidemiology, etiology, and prevention of late IOL–capsular bag complex dislocation: review of the literature. J Ophthalmol. 2015;2015:805706.
2. American Academy of Ophthalmology: Basic Science and Clinical Course. Section 11: Lens and Cataract. 2014-2015;29, 35-38.
3. Carpel EF. Pupillary dilatation in eyes with pseudoexfoliation syndrome. Am J OphthalmoI. 1988;105(6):692-694.
4. Yamane S, Inoue M, Arakawa A, Kadonosono K. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology. 2014;121(1):61-66.
5. Narang P, Agarwal A. Single-pass four-throw technique for pupilloplasty. Eur J Ophthalmol. 2017;27(4):506-508.

