



When complications occur during cataract surgery, it is important to recognize them promptly and strategize their management. This article explores why anterior and posterior capsular tears occur during cataract surgery and how these complications can be managed so that surgery may be completed smoothly and efficiently.
ANTERIOR CAPSULAR TEARS
Sources. The anterior capsule can tear during cataract surgery for several reasons. During the capsulorhexis, the surgeon may lose control of the capsular flap, allowing it to extend. This creates a focal point of weakness in the anterior capsule. (For more on this topic, see "Radialized Anterior Capsulotomy.") A tear may begin at the weak point and progress during subsequent steps of surgery. In an eye with an intumescent white cataract, high lenticular pressure can cause an Argentinian flag sign, where the initial capsular tear propagates rapidly to the periphery of the capsule (Figure 1). At times, an anterior Argentinian flag tear may extend posteriorly.
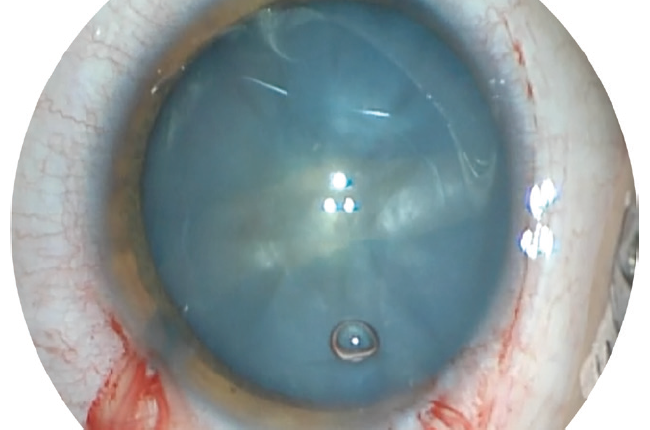
Figure 1. The Argentinian flag sign formed after 180º radialization of the capsulorhexis in an eye with an intumescent white cataract. This tear did not extend posteriorly, and a three-piece IOL was placed in the sulcus. Postoperative UCVA was 20/20.
An anterior capsular tear can also occur during nuclear disassembly if the chopper is positioned improperly (Figure 2). Additionally, without clear visualization of the anterior capsule, the surgeon can inadvertently sculpt the capsule while grooving the lens nucleus.
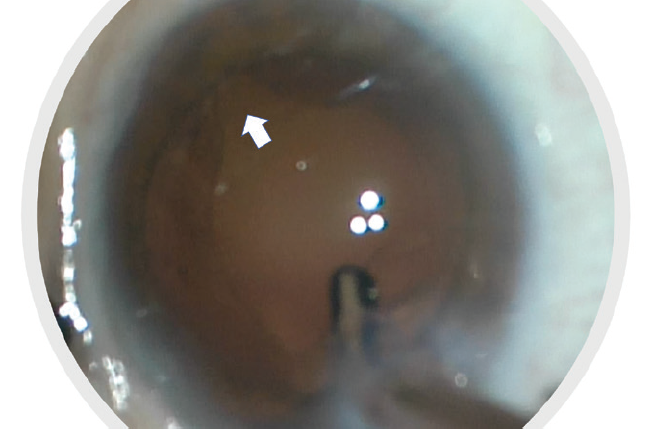
Figure 2. The anterior capsule tore during horizontal chopping of the lens nucleus (white arrow) due to improper placement of the chopper in relation to the anterior capsule.
In an eye with a uveitic cataract, extensive dissection of adherent synechiae off the anterior capsule and manipulation of the iris tissue to achieve pupillary dilation can sometimes disrupt the anterior capsule. If unrecognized, this may cause a capsular tear that can extend progressively during the course of surgery.
Lastly, during cortical removal, excessive pulling of a sticky cortical flap sometimes leads to an anterior capsular tear, which can also extend posteriorly.
Recognition and management. If an anterior capsular tear goes unrecognized, sequelae such as its posterior extension may ensue. If a tear is identified early in a case, infusion pressure should be lowered immediately to reduce stress on the capsular bag and prevent the posterior extension of the tear. During nuclear disassembly, techniques that require frequent rotation of the lens nucleus should be avoided to reduce stress on the anterior and posterior capsules and zonules, especially in the area of the tear. During cortical removal, it is wise to remove cortex in the area of the anterior capsular tear last. Cortex should be pulled toward rather than away from the location of the tear to lessen tension on the capsular bag and prevent a posterior wraparound of the tear.
In the setting of an anterior capsular tear, the capsular bag is generally sufficiently stable to allow the implantation of a one-piece IOL. Compared to a three-piece IOL, a one-piece IOL can be injected into the capsular bag in a more controlled manner, and it tends to unfold more slowly. The IOL is then rotated so that the haptics are oriented perpendicular to the area of the anterior capsular tear. This minimizes stress on that area and avoids further propagation of the tear. If, however, the integrity of the posterior capsule is in doubt, a three-piece IOL should be placed in the sulcus with its haptics located away from the area of the anterior capsular tear. Alternatively, if there is insufficient anterior capsular support, an anterior chamber (AC) IOL may be implanted.
OVD should be removed slowly. Wounds should be hydrated before the I/A handpiece enters or exits the eye to avoid shallowing of the AC (fluctuations in AC fluidics can cause an anterior capsular tear to extend posteriorly). Consideration may be given to suturing the main wound to allow the AC to remain formed postoperatively, and a miotic agent injected intracamerally may help to ensure that the IOL cannot subluxate into the AC.
POSTERIOR CAPSULAR TEARS
Sources. Predisposing risk factors for a posterior capsular rupture (PCR) include poor pupillary dilation secondary to pharmacologic agents, posterior synechiae, or pseudoexfoliation; prior trauma with zonulopathy; a dense lens; a shallow AC; high myopia and a long axial length; prior vitrectomy or intravitreal injection that compromised the posterior capsule; and a corneal opacity that compromises surgical visualization.
When one or more of these risk factors is present, it may be necessary to perform a preoperative peri- or retrobulbar block to achieve adequate anesthesia and akinesia during surgery. Additional sedative agents should be on hand to reduce the patient’s anxiety and pain if necessary. Pupillary expansion devices, capsular tension rings and/or segments, an anterior vitrectomy set, preservative-free triamcinolone acetonide, intracameral miotic agents, and 10-0 nylon sutures should also be easily accessible in the room and ready for immediate use.
Recognition and management. Intraoperative signs of a PCR include sudden and momentary dilation of the pupil, the sudden deepening of the AC, prolapse of iris tissue out of the main wound or paracentesis, altered fluidics in the AC due to the presence of vitreous strands, and posterior tilting or frank posterior dislocation of the lens nucleus.
As with an anterior capsular tear, expedient recognition of a PCR is critical to its successful management. A PCR is most likely to occur after hydrodissection (Figure 3) or during nuclear disassembly or cortical removal (Figure 4). Rarely, a PCR may occur during IOL implantation.
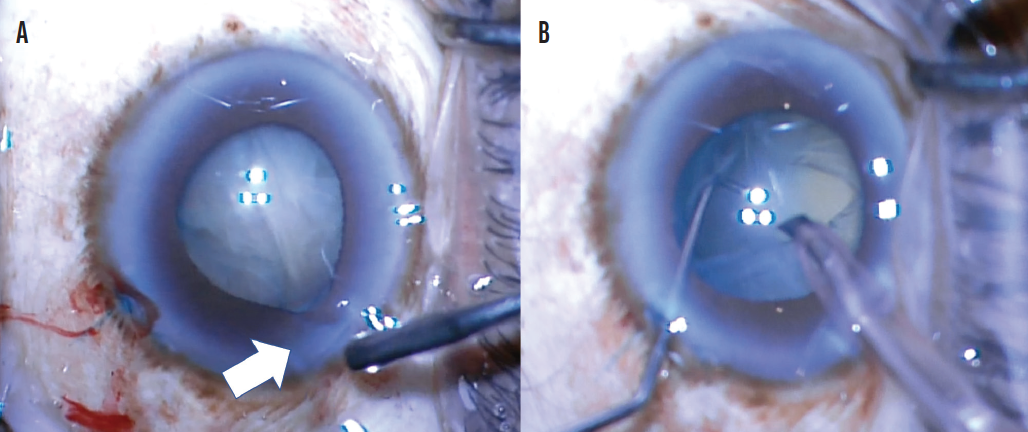
Figure 3. Momentary pupillary dilation with iris prolapse out of the main wound after multiquadrant hydrodissection (white arrow) is suggestive of a PCR (A). After the lens was grooved into two heminuclei, a large horizontal tear of the posterior capsule was noted, and there was complete posterior dislocation of the lens nucleus (B).
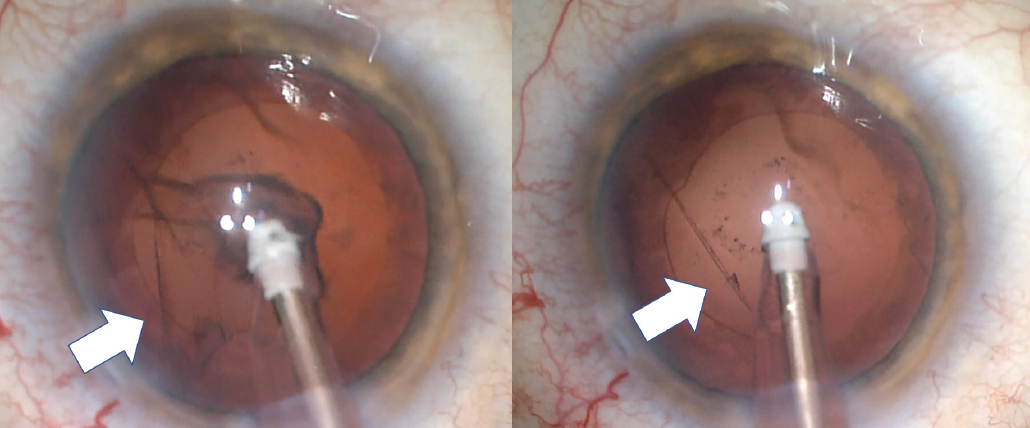
Figure 4. Disinsertion of 5 clock hours of the zonules and the posterior capsule during the removal of adherent cortical material (white arrows) in an eye with ocular graft versus host disease.
When a PCR is detected, a surgeon’s instinct is to remove all instruments from the eye, but this urge must be resisted. Instead, infusion through the phaco handpiece is maintained while a dispersive OVD is injected through the paracentesis into the area of the capsular defect to tamponade the vitreous. Infusion may then be turned off, and the phaco handpiece may be removed from the eye. This chronology prevents a sudden shallowing of the AC that can cause vitreous promptly to prolapse forward.
This is the time in the procedure to pause and assess the situation. If the PCR occurred early in nuclear disassembly, efforts are geared toward safely removing all nuclear fragments and preventing them from falling posteriorly. Caution should be taken to avoid excessive rotation of the lens to prevent propagation of the PCR and a subsequent lack of support for the nuclear fragments. OVD may be used to viscodissect lens fragments into the AC, and phacoemulsification may be performed at or above the iris plane. If vitreous is present in the AC, phacoemulsification should be avoided because it can unnecessarily cause vitreous traction and subsequent retinal tears or detachment. Lens material is viscodissected into the AC angle, and the anterior vitrector is used to cut vitreous strands before phacoemulsification proceeds. Dilute preservative-free triamcinolone acetonide is used to stain the vitreous, and all wounds are checked for vitreous prolapse.
If a substantial amount of nuclear material is present in an eye with a PCR, a lens scaffold technique may be employed. A three-piece IOL is injected underneath the nuclear material to serve as a posterior scaffold above which these pieces can be emulsified or manually expressed through a large clear corneal wound or scleral tunnel. The IOL may then be implanted safely in the sulcus after all of the lens material has been removed.
Once this is completed, a thorough bimanual anterior vitrectomy should be performed through two paracentesis incisions after the main wound has been sutured to ensure adequate AC stability. Cortical removal should not disrupt the anterior capsule, which will serve as a robust scaffold for a sulcus-fixated three-piece IOL with optic capture. If the integrity of the anterior capsule is uncertain, the surgeon must determine if there is sufficient support for the sulcus fixation of an IOL. If there is any doubt, an ACIOL may be implanted. Alternatively, the patient may be left aphakic, and an iris-sutured or scleral-fixated IOL may be placed at a later time.
Often, when a PCR occurs during nuclear disassembly (Figure 5) or cortical removal with the I/A handpiece, there is no vitreous prolapse, and the defect is small. A one-piece IOL can usually be implanted safely in the capsular bag in this situation. OVD should be removed gingerly, and AC shallowing should not be permitted. Otherwise, vitreous prolapse and extension of the tear may occur.

Figure 5. A well-circumscribed circular posterior capsular defect caused by the phaco probe during nuclear disassembly of a soft cataract (white arrow). No vitreous prolapse was detected. Cortical removal was performed safely, and a one-piece IOL was placed in the capsular bag without complication.
At the conclusion of cataract surgery on an eye with a PCR, intracameral miotic agents are instilled, and the pupil is checked for peaking suggestive of residual vitreous in the AC. A circular pupil at the end of the case signals that all vitreous has been removed. Pupillary constriction also prevents postoperative movement of the IOL. Patients should be patched overnight for their comfort. Subconjunctival steroids can be injected to reduce postoperative inflammation.
Postoperative considerations. PCRs and vitreous loss increase the risk of postoperative endophthalmitis. The intracameral injection of an antibiotic and administration of systemic antibiotics may be considered to reduce this risk. Patients require careful monitoring for elevated IOP, macular edema, and retinal tears and detachments. Patients should be seen more often during the first days to weeks after surgery.
One month after surgery, a scleral depressed fundoscopic examination is warranted to rule out retinal pathology, and OCT is recommended to assess the eye for macular edema. Referral to a retina colleague is recommend if there is concern about retinal pathology. Additional topical steroids, NSAIDs, and IOP-lowering agents may be required for patients with any of the aforementioned sequelae.
CONCLUSION
It is important for surgeons to be acutely aware of capsular complications during cataract surgery and to respond with appropriate care and caution (see Key Points). Having multiple plans of action in one’s armamentarium makes achieving an excellent visual outcome more likely.
Key Points
For Anterior Capsular Tears
- Anterior capsular tears can occur at any time during the course of cataract surgery (capsulorhexis, nuclear grooving and disassembly, cortical removal). Expedient recognition of the tear is important to preventing its posterior extension.
- Intraoperative maneuvers to prevent the extension of an anterior capsular tear include lowering the infusion pressure, avoiding excessive rotation of the lens, and pulling cortex toward the area of the tear.
- One-piece IOLs can often be placed in a capsule with an anterior tear. The haptics are oriented perpendicular to the area of the tear.
For Ruptured Posterior Capsules
- The posterior capsule can rupture early or late in the cataract procedure. A plan must be made to remove all lens material and prolapsed vitreous safely.
- A three-piece–IOL scaffold technique may be used if a significant amount of lens material is present when a posterior capsular tear is recognized.
- Dilute preservative-free triamcinolone acetonide should be used to stain the vitreous when performing an anterior vitrectomy. An intracameral injection of a miotic agent can be performed at the conclusion of the case to assess the pupil for peaking, which suggests the presence of residual vitreous in the anterior chamber.

