The safety of modern cataract surgery is undeniable, and thanks to advances in surgical technology and technique, the overall success rate of cataract surgery is 98%.1 In a study of more than 200,000 Medicare beneficiaries, 99.5% of cataract surgery patients experienced no severe postoperative complications.2
As with any surgical procedure, however, risks exist—especially in patients with retinal diseases such as macular degeneration, diabetic retinopathy, and diabetic macular edema (DME). Even when these conditions are identified and managed before cataract surgery, these patients are at increased risk of experiencing complications during and after cataract surgery. This article identifies several approaches that cataract surgeons can take to ensure the best visual outcomes and highest levels of satisfaction after cataract surgery for patients with retinal pathology.
UNDERSTAND PATIENTS’ VISUAL POTENTIAL
As a retina specialist, the best advice I can give to my cataract surgeon colleagues is to ensure that patients with preexisting retinal diseases or conditions are under the care of a retina specialist. If patients have not already seen a retina specialist prior to their preoperative examination, they should be referred for a formal retinal evaluation. The results of this evaluation will provide important information regarding the patient’s visual potential and identify potential risk factors for cataract surgery complications.
The most important part of caring for patients with retinal disease is understanding and communicating appropriate expectations to the patient. Although many patients with retinal conditions will achieve excellent visual quality after cataract surgery, it is important that they understand that their retinal conditions may limit their visual potential, even after perfect cataract surgery. Patients must also understand that their visual recovery may be prolonged and that they will likely continue to require care from a retina specialist after cataract surgery. Coordinated messaging by retina specialists and cataract surgeons can help to ensure that patients have reasonable expectations and receive excellent postoperative care.
Another key element of the preoperative evaluation is discussion with patients about premium IOL options. Premium IOLs have the potential to reduce the need for spectacle correction after cataract surgery. These lenses should be used cautiously in patients with retinal diseases including wet macular degeneration or macular pucker or with a history of macular hole repair surgery. Patients with these conditions may experience distorted or decreased vision due to their macular pathology. It’s important to explain to these patients that neither the cataract procedure itself nor insertion of a premium IOL will improve decreased vision due to their macular condition. Premium IOLs entail an additional out-of-pocket expense for patients, heightening expectations for perfect uncorrected vision after surgery. For this reason, I advise that premium IOLs be used with caution in patients who have known macular diseases.
SURGICAL CONSIDERATIONS
Intravitreal injections with anti-VEGF agents—the standard of care for diseases such as DME, wet age-related macular degeneration, and retinal vein occlusion—is the most commonly performed office procedure in all of medicine. The estimated number of intravitreal injections performed worldwide in 2016 was more than 20 million,3 and that number is on the rise. Patients with these conditions can have successful visual outcomes, but this often requires coordination between the cataract surgeon and the retina specialist.
A common treatment paradigm is to postpone cataract surgery for patients receiving anti-VEGF intravitreal injections until the macular edema or choroidal neovascularization is quiescent. Once the macular disease is quiescent (ie, minimal or no fluid accumulation on examination or OCT), I recommend performing cataract surgery within 1 to 2 weeks of an injection. This will help to decrease the chances of worsening macular exudation or cystoid macular edema in the postoperative period.
Patients with high myopia or a history of retinal detachment also require a preoperative evaluation by a retina specialist because they may be at increased risk of developing a retinal tear or detachment after cataract surgery. A careful dilated examination and peripheral retinal examination to identify retinal pathology such as vitreous traction, lattice degeneration, or an asymptomatic retinal tear or retinal detachment should be conducted before cataract surgery. If pathology is identified, the condition must be treated before cataract surgery is performed, and patients should be advised to monitor themselves for symptoms suggestive of a retinal tear or retinal detachment such as flashing lights, a new onset of floaters, or a loss of peripheral vision.
Some conditions and complications can increase the risk of vitreous loss during cataract surgery. These include pseudoexfoliation, dense white cataracts, eyes that have capsular breach such as postvitrectomy or postinjection, and eyes with zonular loss or lens instability as a result of ocular trauma or certain inherited syndromes (Figure). It is important to discuss the risk of complications and to be prepared to manage them in patients with these conditions. A retinal evaluation is a necessary step before cataract surgery so that the retina specialist can identify and treat any retinal pathology as necessary, counsel patients to be vigilant for symptoms suggestive of a retinal tear or retinal detachment, make them aware of their particular risk factors for complications after cataract surgery, and adjust their expectations for visual recovery as indicated.
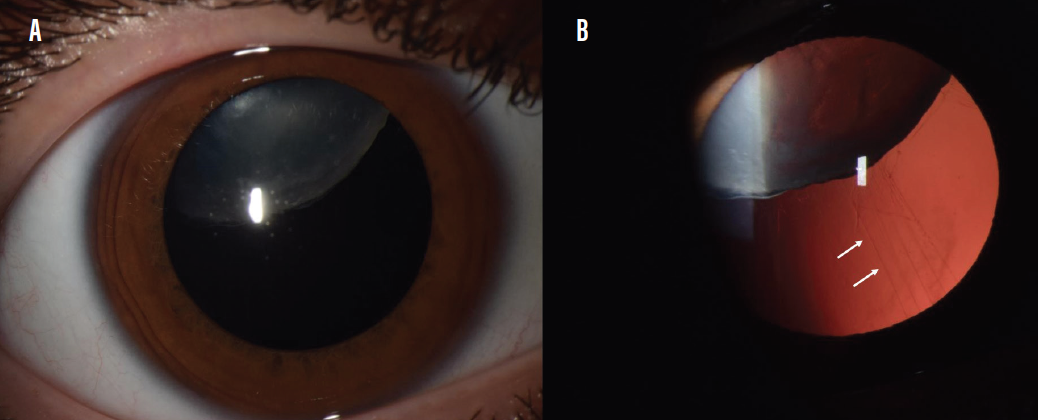
Figure. Subluxation of the opacified crystalline lens in a patient with Marfan syndrome (A). Zonular weakness commonly causes lens instability in this condition (B, white arrows).
Courtesy of Ashley Behrens, MD, and Fernando Arevalo, MD, PhD
For patients at high risk of retinal complications, I also recommend planning cataract surgery with a retina surgeon on standby during the procedure if possible. If there is a problem with the stability of the lens or traumatic zonular loss, for instance, the retina surgeon can assist by removing nuclear fragments that prolapse into the vitreous, potentially saving the patient from an additional surgery.
CONCLUSION
Patients with retinal conditions or risk factors for retinal complications can have successful visual outcomes after cataract surgery. A preoperative evaluation from a retina specialist is essential to identifying underlying risks for potential retinal complications. Thorough documentation and discussion of preexisting visual limitations by both the retina and cataract surgeons help to set realistic postoperative expectations for patients.
Setting appropriate patient expectations and facilitating preoperative retinal evaluation are key to achieving safe, effective surgery in this population.
1. Cataract surgery. Your Sight Matters. Accessed October 26, 2020. https://yoursightmatters.com/cataract-surgery
2. Stein JD, Grossman DS, Mundy KM, et al. Severe adverse events after cataract surgery among Medicare beneficiaries. Ophthalmology. 2011;118(9):1716-1723.
3. Martin DF. Evolution of intravitreal therapy for retinal diseases – from CMV to CNV: The LXXIV Edward Jackson Memorial Lecture. Am J Ophthalmol. 2018;191:xli–lviii.