

Over the past decade and more, cataract surgeons have noticed a shift in patient expectations and demands, with patients more often requesting spectacle independence and maximal acuity across their entire range of vision. As more technologies become available and more resources are accessible to our patients, these expectations will continue to increase.
The current mindset of technology consumers is that a product’s lifespan is only about 1 to 2 years. After that, it is time to upgrade to the next latest-and-greatest technology. As the younger generations start to develop cataracts, they will undoubtedly expect the same potential for upgradability of their lens technology. That is why, in my opinion, exchangeable and adjustable IOLs are the way of the future.
IT STARTS NOW
With current IOL technology, whatever the patient opts for at the time of cataract surgery is a lifetime lens. But even today, some patients ask questions like, “If I get a multifocal IOL now and something better becomes available in the future, could I upgrade my lens?” or “I can’t afford a multifocal IOL right now, but could I exchange it for one in the future?”
Unfortunately, we have to tell these patients no. Because the patient’s lens selection is permanent, it can influence presbyopia-correcting IOL conversion rates. However, if surgeons had the ability to easily exchange a lens—say, when a new technology became available or when a patient was unhappy with his or her vision after surgery—I think it would give them more confidence to offer premium lens technologies and patients more confidence to opt for them.
A NEW SOLUTION
Several adjustable and exchangeable lens technologies are in the pipeline, including the »Gemini Refractive Capsule (Omega Ophthalmics; Figure 1), which I intend to try in the near future. The defined plane in the middle of this implant securely holds a separate IOL in place. The open space could also be used for drug delivery and biometric sensors.

Figure 1. The Omega-4 is the latest design of the Gemini Refractive Capsule.
I envision pairing the Gemini with both traditional and premium lens technologies. I might suggest starting with a monofocal IOL within the Gemini in patients who are not yet ready to invest in a premium lens and then, over time, as their visual or financial status changes, upgrade them to a more advanced IOL. Alternatively, in patients who express a desire for spectacle independence or crisp vision at all distances, I might start with a multifocal IOL now and upgrade to a trifocal IOL technology once one becomes available in the United States.
Another interesting scenario with the Gemini Refractive Capsule is that I could implant the »RxLAL (RxSight) now to give the patient the highest quality distance vision, but in the future exchange that for a light adjustable lens with extended depth of focus.
CLINICAL RESULTS
Gabriel Quesada, MD, recently reported the first human experience with the Gemini Refractive Capsule.1 In the study, the capsule was implanted into the eyes of eight patients at the time of cataract/IOL surgery. Postoperative exams were performed on day 1 and at 1, 3, and 6 months. In all cases, a mild anterior surface iris trauma was noticeable between the pupil and the incision. The anterior chamber depth and shape was normal in all eyes and at all postoperative visits, and Dr. Quesada noted that implantation of the Gemini was technically straightforward.
At 1, 3, and 6 months postoperative, mean distance BCVA was 0.1 logMAR. At 6 months postoperative, four of the eight patients with residual refractive errors elected to receive a secondary IOL to improve UCVA. According to Dr. Quesada, implantation of the piggyback lens was also straightforward. At 1 and 3 months after the piggyback IOL procedure, distance UCVA was 0.13 logMAR.
Dr. Quesada and colleagues concluded that the Gemini Refractive Capsule maintained a large volume of space in the anterior capsule throughout the 6-month period and that the eyes implanted with the capsule had excellent visual acuities (Figure 2).
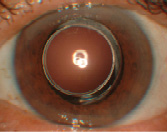
Figure 2. The dilated eye of the first patient to receive the device. At 18 months postop, there was no sign of posterior capsular opacification or adverse effects.
BEYOND TODAY’S TECHNOLOGY
By keeping the anterior capsule open with the Gemini Refractive Capsule, we are essentially providing our patients with the opportunity to later upgrade to lens technologies beyond the refractive technology we have available today.
1. Quesada G. First-in-man experience with a device to maintain an open capsule long-term after cataract surgery. Paper presented at: the 2018 ASCRS meeting; April 16, 2018; Washington, DC.

