



I had the privilege of performing the first single-incision small-incision lenticule extraction (SMILE) procedure in the world, and I have watched this procedure usher in a new paradigm in refractive surgery.
A BRIEF HISTORY OF SMILE
SMILE was developed in 2008 as an extension of the femtosecond lenticule extraction (FLEx) procedure, in which a femtosecond laser was used to cut a flap and a lenticule. The flap was then lifted and the lenticule removed.
AT A GLANCE
- Because SMILE uses a small incision and therefore minimizes the cutting of corneal nerves, studies have suggested that it leads to greater corneal sensitivity and a better tear profile postoperatively compared with LASIK.
- In several published studies, results of SMILE for the treatment of myopia and myopic astigmatism have been equivalent to those for LASIK.
- A multicenter study is under way evaluating SMILE for the treatment of hyperopia, but this treatment modality is not yet available to surgeons outside the trial.
In SMILE, the flap is replaced with a small incision. The surgeon uses the »VisuMax femtosecond laser (Carl Zeiss Meditec) to cut both surfaces of a lenticule within the cornea (Figure 1). The lenticule shape is determined by the eye’s refractive error. The surgeon then removes the lenticule through a small incision that was also made by the femtosecond laser when the lenticule was created (Figure 2).
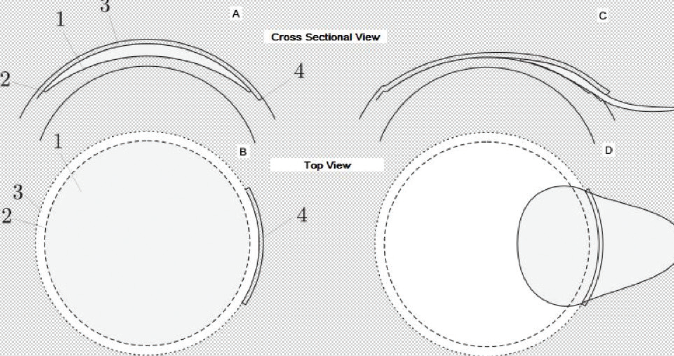
Figure 1. The cross-sectional and top views of the cuts involved in the SMILE procedure.

Figure 2. The SMILE procedure: The VisuMax laser cuts both surfaces of a lenticule within the cornea (A); the lenticule is removed through the small incision that was made when the lenticule was created (B-E).
SMILE offers several advantages over femtosecond LASIK (see SMILE vs LASIK below). Since 2008, the procedure has seen several refinements. The laser delivery has been improved in a number of ways to decrease visual recovery time: The scanning direction of the laser was changed, the laser speed was increased from 200 to 500 kHz, the spot energy was decreased, the spot and track distances were changed, the instrumentation required for separation and removal of the lenticule has been refined, and the shape of the lenticule and the way astigmatism was corrected were changed to improve results in the treatment of astigmatism. Further, several surgeons have developed techniques to compensate for cyclorotation of the cornea in the treatment of high astigmatism.
SMILE VS LASIK
SMILE has several advantages over femtosecond LASIK:
- It requires only one laser, which reduces both capital costs and the cost per procedure;
- It improves workflow because the patient does not need to move from one laser to another;
- The total energy used in SMILE is less than is used in femtosecond LASIK;
- Because the procedure involves cutting rather than ablation, there is less scatter in the results, as ablation rates are dependent on factors such as the hydration level of the cornea; and
- The small incision opens the possibility of better biomechanical stability and fewer dry eye symptoms postoperatively.
The range of treatments used to be from spherical equivalent of -0.50 D to -10.00 D of myopia. The upper range has now been increased to -12.50 D (Editor’s note: outside the FDA-approved range in the United States). With more refined instrumentation, the incision size has also been reduced. Many surgeons, myself included, now remove the lenticule through a sub–3-mm incision.
Initially, retreatments with SMILE were a concern, but for several years now software on the VisuMax laser has allowed surgeons to convert the SMILE cap into a flap (Editor’s note: This software is not yet available in the United States). Retreatments with an excimer laser are then possible after lifting the flap. Techniques are also being developed to perform enhancements using only the femtosecond laser.
STUDY FINDINGS
In several published studies, results of SMILE for the treatment of myopia and myopic astigmatism have been equivalent to those for LASIK.1 Studies have also reported better results in high myopia with SMILE than with conventional femtosecond LASIK.2 Other studies have found that the amount of wavefront aberrations induced after SMILE were less than or equivalent to those induced by wavefront-compensated femtosecond LASIK.3
A multicenter study is under way evaluating SMILE for the treatment of hyperopia, but this treatment modality is not yet available to surgeons outside the trial. Many surgeons have attempted to preserve the lenticules that are removed during SMILE. The lenticules have then been used to treat hyperopia by inserting the lenticule into a pocket created in the cornea with a femtosecond laser. Another use of the lenticules has been to enhance the biomechanical strength of corneas with ectatic disease.
Because SMILE uses a small incision and therefore minimizes the cutting of corneal nerves, studies have suggested that it leads to greater corneal sensitivity and a better tear profile postoperatively compared with LASIK. This is a major benefit of SMILE and a reason why many patients find the procedure attractive.
SUMMARY
SMILE obtained FDA approval for the treatment of myopia in 2016. Since then, it has become popular in the United States. Worldwide, more than 1 million SMILE procedures have been performed to date. The procedure is well on the road to changing the way that refractive surgery will be performed in the future.
1. Zhang Y, Shen Q, Jia Y, Zhou D, Zhou J. Clinical outcomes of SMILE and FS-LASIK used to treat myopia: A meta-analysis. J Refract Surg. 2016;32:256-265.
2. Vestergaard A, Ivarsen A, Asp S, Hjortdal JØ. Femtosecond (FS) laser vision correction procedure for moderate to high myopia: a prospective study of ReLEx flex and comparison with a retrospective study of FS-laser in situ keratomileusis. Acta Ophthalmol. 2013, 91(4):355-362.
3.Agca A, Demirok A, Cankaya KI, et al. Comparison of visual acuity and higher-order aberrations after femtosecond lenticule extraction and small-incision lenticule extraction. Cont Lens Anterior Eye. 2014; 37:292-296.

