

The holy grail of cataract surgery is to match the accuracy of laser refractive surgery and allow patients to attain maximal postoperative visual outcomes. However, a recent report including more than 200,000 eyes found that only about three in four were within ±0.50 D of predicted spherical equivalent after cataract surgery.1 Roberts and coworkers reported similar results using advanced IOL calculation formulas.2 These results indicate a need for technological improvements in the area of cataract surgery refractive outcomes.
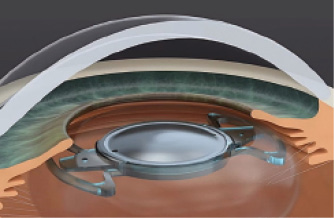
Figure 1. Illustration showing the Precisight IOL implanted in the capsular bag.
A new generation of modular and multicomponent IOLs has the potential to accurately and safely resolve these postoperative refractive issues. One such multicomponent IOL is the Precisight system (InfiniteVision Optics).3,4 It consists of two refractive lenses (Figure 1), a front and base lens, which are preassembled outside the eye (Figure 2). This assembled complex is then injected into the capsular bag through a 2.2-mm clear corneal incision. Together, both lenses provide the refractive power needed by the eye (Figure 3).
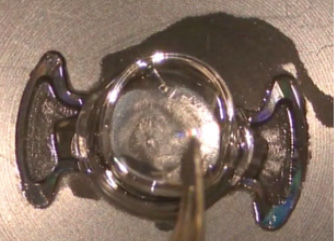
Figure 2. Surgical microscope view of the front of the lens being attached to the bridges of the base lens before implantation.
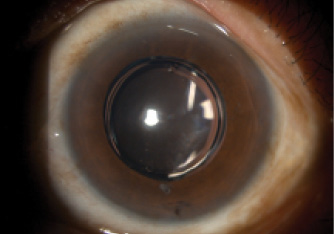
Figure 3. Slit-lamp photograph of the Precisight IOL at 3 months after implantation. Note the absence of capsular folds and posterior capsular opacification.
In the event of a refractive surprise or other optical issues, the front lens can be removed and exchanged for a new front lens with a different refractive power in a 5-minute surgical procedure (Figure 4). A major advantage of this system lies in the ease of implantation during the primary procedure, similar to that of conventional IOL implantation. The workflow in the OR is thereby unaltered.
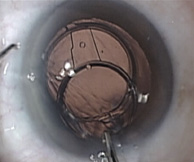


Figure 4. Surgical microscope view of the enhancement procedure. IOL forceps are used to grab one tab and pull the front lens out of the eye through the original main incision site (top). A new front lens with correct dioptric power is injected through the original main incision site into the anterior chamber; a Sinskey hook is used to guide the tabs into both bridges of the base lens (middle). Enhancement procedure is complete, with the new front lens secured by the base lens bridges. There is no change in the IOL axis after enhancement (bottom).
CLINICAL EXPERIENCE
I have performed more than 50 front lens exchanges with the Precisight at 3 to 7 months after primary surgery. After the enhancement, UCVA in 100% of these eyes has been 20/25 or better. The mean manifest refraction spherical equivalent of 1.39 D before enhancement decreased to 0.09 D after enhancement. The lens position is predictable, and there is excellent rotational stability.
During the enhancement procedure, the front lens tabs are easily separated from the base lens using simple instruments. IOL forceps are then used to pull the front lens out of the eye through the original main 2.2-mm incision without the need for cutting the IOL. A new front lens is inserted into the position of the extracted front lens.
With conventional IOLs, there is a race against time for IOL exchange because capsular fibrosis can complicate the exchange process. However, with the Precisight, the enhancement procedure is unaffected by capsular fibrosis and time elapsed after primary surgery.
UTILITY AND APPLICATION
Multicomponent IOLs such as the Precisight will be helpful for patients with high visual expectations or for those with a high likelihood of refractive surprise, such as eyes with previous refractive surgery, corneal transplantation, or extreme ocular dimensions. Further, surgeons will be able to easily exchange a multifocal IOL for a monofocal if patients experience poor tolerance or visual disturbances. The exchange can be performed without time limit, providing patients with the maximal period for neural adaptation. The Precisight also provides the opportunity for long-term enhancements when a change in refraction occurs. The Precisight has received the CE Mark and is commercially available in Europe.
1. Lundstrom M, Stenevi U, Rosen P, et al. EUREQUO annual report 2016: cataract and refractive surgery in 2016 as reflected by the EUREQUO database. Paper presented at: Congress of the European Society of Cataract and Refractive Surgeons; October 7-11; Lisbon, Portugal.
2. Roberts TV, Hodge C, Sutton G, Lawless M. Comparison of Hill-radial basis function, Barrett Universal and current third generation formulas for the calculation of intraocular lens power during cataract surgery [published online ahead of print August 31, 2017]. Clin Exp Ophthalmol.
3. Fuchs HA, Frohn A, Dean K, Werblin TP. Multiple component intraocular lens: first human implantation. J Refract Surg. 2009;25(4):390-393.
4. Portaliou DM, Grentzelos MA, Pallikaris IG. Multicomponent intraocular lens implantation: two-year follow-up. J Cataract Refract Surg. 2013;39(4):578-584.

