For the past 5 years, ophthalmologists have had access to the femtosecond laser to assist with cataract surgery. Whereas the software of the available platforms seems to be updated on a weekly basis, helping to refine energy levels, incisional architecture, and safety, one aspect of laser cataract surgery remains unchanged: the ophthalmologist must safely remove the cataract manually. Laser pretreatment changes the look and feel of cataract surgery in many ways. This article shares some pearls to ease the learning curve when combining femtosecond lasers and phacoemulsification.
THE PUPIL
One advantage of the laser is its ability to make a capsulotomy and presoften the lenticular material. Making sure the pupil is large enough at the time of laser application and maintaining dilation for the remainder of surgery are essential. Delays in the surgical schedule owing to slow pupillary dilation are frustrating. In patients for whom blood pressure is not an issue, instilling a drop of 10% phenylephrine in the operative eye may assist in enlarging the pupil to a treatable size. In many cases, I have instructed patients to use cyclopentolate 1% in the operative eye starting 2 hours prior to surgery.
AT A GLANCE
• Many cataract surgeons have embraced the use of a femtosecond laser, but some have been frustrated by changes in the “feel” of the necessary phacoemulsification.
• Making sure the pupil is large enough at the time of laser application and maintaining dilation for the remainder of surgery are essential.
• Early in the transition to laser cataract surgery, it is helpful to make nuclear removal feel as familiar as possible. The author recommends that surgeons continue to use their standard technique and ignore the fragmentation lines created by the laser.
• One of the most notable differences in laser versus traditional cataract surgery is cortical cleanup.
Particularly when there is a delay before the phacoemulsification, miosis of the pupil can occur after laser treatment, although an improvement in laser profiles and lower energy settings have reduced the incidence of this problem. Although an additional drop of phenylephrine after laser treatment can help, this measure may not suffice. It is therefore advisable to have access in the OR to a dilating agent for intracameral use. It may be in the form of compounded preservative-free epinephrine or a combination of lidocaine and epinephrine (Shugarcaine). I have been using Omidria (Omeros), which is a combination of ketorolac and phenylephrine added to the irrigating solution that is FDA approved for maintaining pupillary dilation.
In rare cases, the pupil resists pharmacologic dilation, and an expansion device becomes necessary. Special care is required when placing a ring or iris hooks to avoid engaging the edge of the capsulotomy. My preferred technique is to elevate the iris off the lens’ surface with an ophthalmic viscosurgical device and then carefully place each hook or scroll of the pupil expander while visualizing the edge of the capsulotomy. I find that this technique helps to ensure that only the pupil is expanded, not the capsulotomy.
CAPSULOTOMY
With laser cataract surgery, the ophthalmologist must transition from a capsulorhexis to a capsulotomy. Although the laser may simplify the capsulotomy’s creation, changes in surgical technique are necessary for the cataract’s safe removal. When first performing laser cataract surgery, ophthalmologists will immediately notice that the familiar red reflex is gone, replaced by a yellowish reflex and a lens and anterior chamber filled with air bubbles. The loss of the red reflex makes visualization of the capsulotomy more challenging.
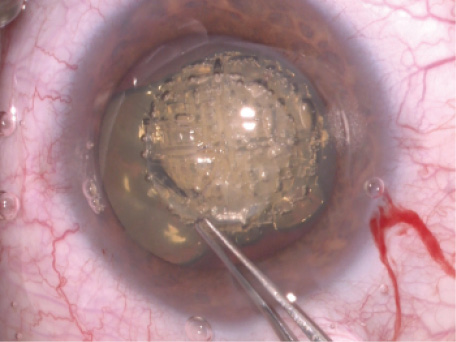
Figure 1. Use of a Utrata forceps to help ensure a complete capsulotomy by replicating the tearing motion of a capsulorhexis. Note the lack of a red reflex because of gas captured in the lenticular material.
Most of the time, the capsulotomy is complete, but rarely, small adhesions remain. Until the surgeon feels confident with this step, I recommend grasping a free edge of the capsule and simulating the tearing motion as if making a capsulorhexis to ensure that there are no attachments and that the capsulotomy is complete and intact (Figure 1).
HYDRODISSECTION
When I began performing laser cataract surgery, I was overly cautious with hydrodissection, which led to difficult lens rotation. Less aggressive hydrodissection is adequate when using a laser, but some level of dissection remains helpful. In my experience, gentle pressure on the lens itself allows some of the gas trapped in the lenticular material to escape, thereby making room for a fluid wave. After releasing a bubble or two, I perform gentle hydrodissection in two or three quadrants along the anterior capsulotomy. I do not always see a fluid wave, but with the help of the pneumodisscetion, the lens still rotates easily.
NUCLEAR REMOVAL
Early in the transition to laser cataract surgery, it is helpful to make nuclear removal feel as familiar as possible. I recommend that surgeons continue to use their standard technique and ignore the fragmentation lines created by the laser. As their experience and comfort level grow, ophthalmologists will naturally incorporate the fragmentation pattern into their lens removal technique.
The pattern of lens softening can also be modified to complement the surgeon’s preferred nuclear removal technique. Those who favor divide and conquer or vertical chop may prefer to simply add “chop” lines instead of relying on diffuse grid patterns, which could make the purchase of lenticular material more difficult. Once comfortable with how the laser changes the feel of nuclear disassembly, surgeons can make modifications to further customize nuclear removal.
CORTICAL CLEANUP
One of the most notable differences in laser versus traditional cataract surgery is cortical cleanup. The laser cleaves several hundred microns of cortical fibers under the capsulotomy, leaving a clean edge of cortex under the anterior capsule. With no wisps of cortical material, it can be difficult to recognize where the cortical material is. I recommend placing the tip of the I/A unit under the anterior capsule under gentle vacuum. Next, the surgeon carefully engages the cortical fibers and initiates aspiration once confident that only cortex (not capsule) is in the aspiration port. After the first strip of cortex is removed, the remainder is much easier to address. Use of bimanual I/A also greatly simplifies cortical cleanup in laser cataract surgery (Figure 2).
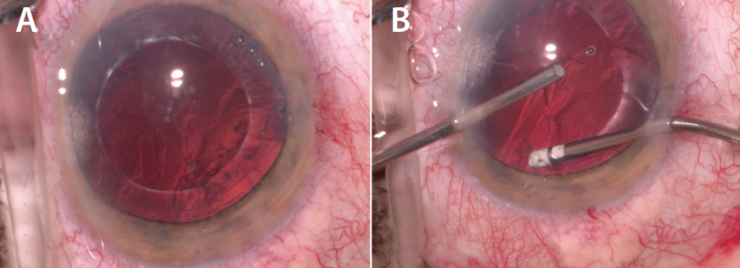
Figure 2. Note the lack of wisps of cortical material extending beyond the laser capsulotomy (A). Use of a bimanual I/A unit to assist with cortical cleanup in laser cataract surgery. Note the two sideport incisions for the bimanual technique (B).
CONCLUSION
Many cataract surgeons have embraced the use of a femtosecond laser, but some have been frustrated by changes in the feel of the necessary phacoemulsification. I hope that these suggestions for managing the pupil, capsulotomy, and nuclear removal ease the transition to laser cataract surgery.