CASE PRESENTATION
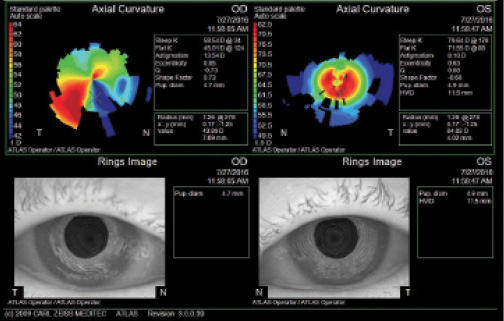
Figure 1. Topography (Atlas 9000 Corneal Topography System; Carl Zeiss Meditec) shows severe irregular astigmatism in both eyes and ectasia in the left eye.
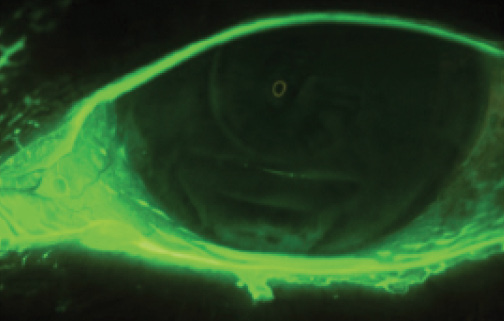
Figure 2. Fluorescein staining of the left eye with slit-lamp photography.
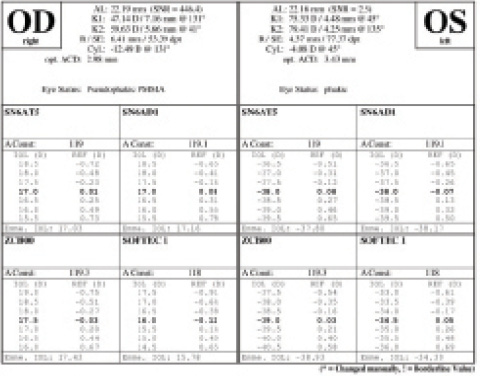
Figure 3. IOLMaster biometry of the right and left eyes.
—Case prepared by Salomon Esquenazi, MD,
and Moises Enghelberg, DO.

AUDREY R. TALLEY ROSTOV, MD
There are two separate issues here. The first is the left eye’s highly irregular cornea and cataract. The second is the failed, vascularized graft in the patient’s right eye.
Regarding the right eye, the patient may be able to undergo simple limbal epithelial transplantation if there is significant ocular surface vascularization, followed by either Descemet stripping endothelial keratoplasty or repeat PKP. This strategy is a reasonable consideration if the right eye has undergone only one transplant procedure to date. Many grafts fail because patients do not adhere to prescribed therapy with topical steroids and/or keep follow-up appointments—points to consider.
There are two possible approaches to the left eye. With the patient’s history of ALK and central hexagonal keratotomy, it should be possible to perform a deep anterior lamellar keratoplasty (DALK) procedure, which would regularize the cornea and decrease the risk of rejection. I would explain to the patient the difference between performing a partial-thickness DALK versus a PKP. If she were amenable, I would perform femtosecond laser-assisted DALK on her left eye. After the cornea achieved refractive stability in 6 to 12 months, I would perform laser cataract surgery, most likely followed by implantation of a toric IOL. I believe that this sequence of procedures would provide the patient with the best visual outcome.
Another option would be to see how a scleral contact lens fit in her left eye. If this modality were successful, the surgeon could consider cataract surgery for the patient’s left eye, followed by a scleral contact lens. In my experience, patients with a history of ALK do not fare well with cataract surgery alone but return for a transplant, followed 6 to 12 months later by an IOL exchange using a piggyback lens.

JODI I. LUCHS, MD
In this case, I think less is more. Because the patient does not want a PKP, I would first consider cataract surgery on the left eye with the IOL power based on her axial length, followed by fitting with a scleral lens, assuming the central cornea was clear.

SHERI ROWEN, MD
I hope this type of case does not become all too common in the future. The high minus powers of available IOLs go to -10.00 D. I once had a patient whose refractive error was left at -15.00 D by another cataract surgeon to match the myopia in the contralateral eye. In that case, I inserted a Visian ICL (STAAR Surgical) anterior to the IOL, which gave the patient 20/20 UCVA. Of course, that patient’s corneas were normal. I also achieved a successful result with the Visian ICL, however, in a patient with a highly irregular cornea after PKP.
I would recommend trying a scleral contact lens in this case if the cornea cannot be improved, and I would keep the Visian ICL in mind as a piggyback option.

DAN B. TRAN, MD
I will focus my discussion on the left eye, as suggested. I successfully treated a similar patient; the K reading was only in the high 50s, however, and the cornea was not as irregular. In that case, I first sent the patient abroad for a topography-guided PRK (not FDA approved at the time). Six months later, I performed cataract surgery and implanted a -10.00 D IOL AR40M IOL (Abbott). The patient did well, with 20/50 UCVA and 20/40+ BSCVA (-0.25 -1.50 × 070).
In this case, I would first test the patient’s tolerance of a scleral contact lens. If she did not tolerate the lens, I would consider corneal collagen cross-linking and possible topography-guided PRK to reduce the irregularity of the central area. This would only work if reproducible topographic measurements could be obtained. A discussion of corneal haze and progressive ectasia would be a part of the informed consent process. I would then wait 3 to 6 months before performing cataract surgery. Biometry using the IOLMaster would not be accurate for IOL selection. The patient will probably need a high-minus lens; the AR40M IOL is available in high-minus powers. I would attempt intraoperative aberrometry but anticipate not being able to capture images.
If the patient tolerated a scleral lens, I would just perform cataract surgery to avoid all of the potential complications with corneal procedures.
Another option would be a possible a 7.75- to 8-mm PKP performed first; I would avoid a 9-mm PKP with its associated higher risks of rejection owing to the proximity to the limbus. DALK could also be attempted and converted to a PKP if perforation occurred. Based on the patient’s experience with her right eye, she most likely will not consent to a corneal transplant procedure. Cataract surgery could be performed 3 to 6 months after PKP. If the first option failed, then this might be the only viable alternative.

KENNETH A. BECKMAN, MD
My first step would be cataract surgery, and I would leave the left eye aphakic, because the IOL power calculations will not be accurate. I would check the patient’s manifest refraction at 1 week and consider a secondary IOL based on the postoperative examination. At this time, I would conduct a scleral lens trial to see what the potential visual acuity was through the cornea after cataract removal. If that refraction were accurate, I would perform IOL calculations based on that refractive information. If an improvement in vision could not be attained with a scleral contact lens, it would become necessary to consider a cornea-based procedure, which should be discussed prior to any intervention.

JEFFERY WHITMAN, MD
Stepping back from the patient’s opinions, I always like to pick the best procedure for correcting the problem. In this case, that is a PKP. I do not know what the circumstances for failure were in the right eye. The left eye’s topography is highly irregular, and I believe replacing the cornea with a full-thickness procedure will provide the best chance of normalizing its shape. A PKP combined with cataract surgery or performed separately to better determine IOL power would be my recommendation.

DAVID J. SCHANZLIN, MD
This patient’s problems stem from the original, poorly conceived surgeries—hyperopic ALK and the secondary trapezoidal keratotomy—which led to her ectasia. PKP was the correct procedure for the right eye, and the 9-mm sizing was most indicated, owing to the ectatic process. The cause of graft failure might be multifactorial, and I would first do what could be done for the right eye. Although the option of endothelial keratoplasty surgery could be entertained, I would more likely use a smaller graft (eg, 7 mm) to clear the central optical zone. I suspect that using the tectonic first graft will produce less astigmatism in the new, smaller transplant.
As far as the left eye, I would be concerned with a topography-guided PRK. The cornea is ectatic and too steep and irregular to be the backbone of an IOL calculation. For this reason, I would perform PKP first and, once the corneal cylinder stabilized, proceed with secondary cataract surgery.
I have a final comment with regard to the use of a toric IOL in PKP cases. I have seen more than a handful of patients over the past year who were referred for management after surgeons implanted toric IOLs in eyes that clearly were going to need a contact lens to see well postoperatively. To my mind, it is best to determine what type of lens fit can be obtained preoperatively with an RGP or scleral lens to improve postoperative outcomes.


WHAT WE DID: SALOMON ESQUENAZI, MD, AND MOISES ENGHELBERG, DO
We understood from the beginning that a 75.00 D cornea cannot create a satisfactory optical image, and we tried our best not to compound the problem. We planned to perform a PKP followed by cataract surgery as a two-stage procedure. We did not consider DALK surgery, which has reduced chances of rejection, because of the significant trapezoidal keratotomy, with long 5-mm central incisions present at the 5-mm optical zone. Based on the patient’s great reluctance to undergo PKP, however, we first tried fitting her with a BostonSight PROSE scleral lens (BostonSight). Our thought was that, if the patient could tolerate the lens, she could undergo a simple cataract surgery. The device vaults the entire cornea and limbus, bathing them in a pool of nonpreserved sterile saline, while at the same time optically neutralizing irregular astigmatism. Each scleral lens is custom fitted by means of a series of casts via which the final ocular prosthesis is refined.1,2
In South Florida, we are lucky to have amazing scleral lens fitters. The device fitted had a base curve of 7.67 mm, a spherical power of +2.75 D, and a diameter of 15.6 mm. The patient was able to wear the lens comfortably all day long. We remeasured her biometry while she wore the scleral lens. This time, we obtained a reading of K1: 46.95 D/7.19 mm and K2: 45.14 D/7.48 mm with astigmatism of -1.81 D. This measurement called for a 23.00 D hydrophobic acrylic IOL. We selected a lens with positive asphericity to counter the high negative asphericity caused by central corneal steepness. The patient underwent cataract extraction by phacoemulsification without complication.
Postoperatively, we referred the patient to the scleral lens specialist, who refitted her based on the new refraction. The parameters of the new lens were a base curve of 7.67 mm, a spherical power of +5.75 D, and a diameter of 15.6 mm. The patient’s final BSCVA was 20/50 OS. She currently uses her scleral lens all day without difficulty and is able to perform all activities of daily living.
Editor’s note: the FDA did not approve topography-guided PRK for abnormal corneas.
1. Schein OD, Rosenthal P, Ducharme C. A gas-permeable scleral contact lens for visual rehabilitation. Am J Ophthalmol. 1990;109(3):318-322.
2. Baran I, Bradley JA, Alipour F, et al. PROSE treatment of corneal ectasia. Cont Lens Anterior Eye. 2012;35:222-227.