
After 2 years of running a dedicated dry eye clinic in northern New England, I (E.J.) continue to contend that managing dry eye disease (DED) and common related ocular surface problems is among the greatest of practice opportunities for eye care providers today. Most surgeons are aware of the importance of ocular surface health as it pertains to consistently excellent surgical outcomes and therefore to creating and retaining happy patients. Because meibomian gland dysfunction (MGD) is a primary cause or contributor in upward of 85% of DED cases,1 equipping your clinic with the equipment to diagnose and treat MGD—and your staff with the understanding they need to discuss this common ocular condition—is crucial. I have found that providing DED-related services and ongoing care to these patients is both professionally and financially rewarding.
DED EXPERTISE
I have established my practice as a dry eye center of excellence, although I have separated this center from my general ophthalmology practice. (I staff the dry eye clinic in a satellite office, 1 to 2 days a week.) Having an office dedicated to DED care allows patients to experience their care as “special.” Like with the cosmetic-oculoplastic care I provide, I find that patients relate better to an office that is focused solely on their concerns. It is useful to note that the demographic suffering from DED substantially overlaps the cosmetic demographic.
When a patient presents to my general practice and is diagnosed with DED, the staff and I inform him or her of our intensive focus on this area. Basic questionnaire and technician-driven screening, followed by tear osmolarity testing, is a routine part of this initial evaluation and is covered by most insurance providers. I use this opportunity to explain the basic problem of ocular dryness. I also quickly and efficiently screen the appearance of the meibomian glands using transillumination and probe their function using a cotton-tipped applicator rolled against the lid margin to attempt meibomian gland expression. My staff and I explain that there are new technologies available to further diagnose and treat DED. Patients are educated that the technology we provide is cutting edge, which sometimes means it is not yet covered by insurance, and we are able to provide new ways of managing their DED that may not be available at other practices. If the patient seems interested, we provide specific details about the cost and nature of the procedures and technology we offer. This process of screening patients provides a steady stream of individuals to the DED clinic, with each of them already prepared for a more intensive examination and likely treatment on the same day.
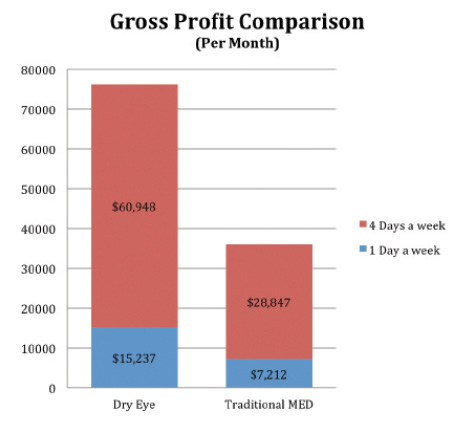
Figure 1. A comparison of Dr. Jaccoma’s typical DED income (over the past year) to that of non-DED medical practice income.
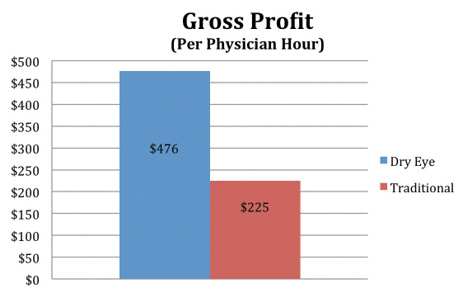
Figure 2. The profitability of DED therapies can be significantly higher than that of traditional ophthalmology when assessed as gross profit generated per physician hour.
Fortunately, most insurers now commonly cover many of the more important diagnostic tests we use. Our practice charges a nominal fee for LipiView and the Meibomian Gland Evaluator (both from TearScience), as they are not covered services, but useful for educating patients about their poor blinks and insufficient tear oils. We include Schirmer testing as a normal part of the DED examination. Patients may opt out of tests not covered and still avail themselves of other insured tests such as the Keratograph (Oculus), noninvasive tear breakup time, tear meniscus and fluorescein staining photography (most insurance pays for the photography-related diagnostic testing), and InflammaDry (Rapid Pathogen Screening). At this dry eye-focused examination, I evaluate and grade all aspects of DED and ocular surface disease, including conjunctival chalasis, lid malpositions, pterygia, and other ocular surface problems.
In full disclosure, I should note that performance of all this extra testing will do little more than cover the expenses of this diagnostic technology. The “payoff” comes from what you do with this information. First, it is useful to keep any other ocular and systemic illnesses in mind. A low Schirmer score coupled with a history of dry mouth will lead to a rheumatology-directed screening for Sjögren syndrome and potentially save a life (treatment may lessen the related incidence of lymphoma). Second, concomitant use of glaucoma medications (common to this demographic) may lead to selective laser trabeculoplasty in an effort to reduce the side effects of these medications and/or preservatives exacerbating their DED. Third, findings of coexisting cataract may lead to combined surgery with an iStent Trabecular Micro-Bypass Stent (Glaukos) for the same reason. Fourth, eyelid malpositions bounce patients back to the general clinic for corrective procedures, and significant pterygia may require excision. Needless to say, the surgical outcomes for cataract and pterygia are less satisfactory when coexistent DED conditions are not adequately addressed. Ptosis or aggressive blepharoplasty repair can only make active DED problems worse, so surgical outcomes can be substantially improved by adequately dealing with the DED issues first. Fifth, good correction of DED may make premium IOL or laser vision correction choices available to a greater number of patients than otherwise possible. These new options open the door to the dry eye-related contact lens-intolerant patients’ finding renewed interest in their optometrist’s contact lens care. This can earn a new pathway for optometric referrals, which can grease the wheels for greater access to all aspects of surgical eye care. Finally, in concert with a group of forward-thinking individuals, I have cofounded a company we call eyeThera. A goal of this company is to market the homework we feel is necessary to help address the common pitfalls resulting in DED. The ongoing revenue from kit sales is another source of income, while also facilitating the restitution of adequate tear function.
What will truly and more directly pay for the added overhead of this clinic is the added income from the DED-related services you can provide. It used to be that a prescription for Restasis (cyclosporine ophthalmic emulsion 0.05%; Allergan) and a set of punctal plugs or punctal hyfrecation was about all most dry eye clinics could provide as an additional reimbursable service. Although this technology remains useful, the rest of the DED landscape has completely changed. With the advent of LipiFlow (TearScience) to restore meibomian gland function, we now have an FDA-approved, well-studied, and clinically proven treatment for up to 85% of our DED patients.2-5 Average net income per bilateral treatment is close to cataract reimbursement for this 12-minute, in-office, painless procedure used to cap off a substantial number of these new MGD patient encounters. For those with significant ocular rosacea, I will often couple this—or primarily treat—with Dr. Roland Toyos’ intense pulsed light (IPL) procedure. Like LipiFlow, the Dermamed IPL treatment can offer an additional opportunity to rejuvenate lower lid meibomian glands with each of the four consecutive, monthly treatments, while helping to close the inflammation-bearing blood vessels that patients dislike for the rosy, ruddy complexion they cause. Although this can net closer to $2,000, it requires a bit more professional time in manually expressing the IPL-treated glands and is considerably more uncomfortable for the patients due to this significant eyelid pressure. It also opens the door to the opportunity for general complexion treatments of the face, neck, and décolletage areas for those who find the midface results compellingly beneficial. Problems like rosacea are chronic and progressive, so patients need to understand that maintenance treatments will be necessary (which can also amount to $500-$1,000 per patient per year in ongoing treatments). I include a starter kit with my LipiFlow and IPL services, to aid in recovery from MGD and to set the stage for the continued use of the kit’s contents.
Treating conjunctival chalasis after dealing with dysfunctional tears helps to maximize the benefit of these healthier tears by allowing them to more easily cover the entire ocular surface with every blink. I explain to patients that the increased surface area and distraction and disruption of the tear film caused by this condition can frequently be reversed with a brief, in-office application that is usually covered by their insurance. I favor the technique of Steve Safran, MD.6 I perform a modified version of his procedure, which you can watch here: eyetube.net/?v=ipene. I should add that the Current Procedural Terminology code is 68330 for the International Classification of Diseases 9 diagnosis of 372.81. Check with a local carrier to see whether this is a covered service and how much they will pay for it. If a patient cannot afford the recommended treatments in our DED practice, then we will continue to treat him or her within the medical insurance arena to the best of our abilities.

FINANCIAL BENEFITS
Limited Medicare compensation rates have been putting significant strain on many small practices, and mine has been no exception. By investing in DED treatments, I have not only acquired more therapies that I can now draw from when treating suffering patients, but also, the investments that I have made in DED have proven to be financially viable. Figure 1 provides a gross profit comparison of my typical DED income (over the past year) to that of my non-DED medical practice income. The profitability of DED therapies can be significantly higher than that of traditional ophthalmology when assessed as gross profit generated per physician hour (Figure 2).
EDUCATING PATIENTS
Our practice also hosts patient education forums. At these and in one-on-one interactions, I explain how the meibomian glands can gradually become atrophic and wither away. If not effectively treated, we can lose the ability to rejuvenate the gland. I present enough basic science to help patients understand why it is important to be treated, and when appropriate to their disease, we give them this information as a call to action.
OUTREACH PROGRAM FOR ODs and MDs
We also hold forums to educate other health care professionals, optometrists and fellow ophthalmologists, in particular. This will help them identify and refer patients and equip them with the tools to monitor patients after I have treated them, facilitating integrated care of DED. I actively encourage optometrists to refer patients to our practice and to get more involved in the process. If all eye care providers have the same level of understanding of MGD as we do, they are more likely to make appropriate referrals. When patients need an ophthalmologist’s level of care, however, such as more invasive treatments (lid surgery, conjunctival chalasis surgery, etc.) or more thermal pulsation system treatment, they will return to our practice. Educational outreach to optometrists and ophthalmologists is ongoing so that we all understand more about the problem and what the full range and capability of treatment can be.
CONCLUSION
The meibomian glands are a separately functioning unit that have their own life cycle, ups and downs, and potential pitfalls, and until patients and physicians truly understand the critical importance of these glands and their function in ocular surface health, tear stability, and balance, they will not truly understand DED. Ocular surface and lid issues play substantially important roles. Using existing tools, we can treat many aspects of DED, making for better outcomes, happier patients, and a more solid bottom line for our practices. n
1. Lemp MA, Crews LA, Bron AJ, et al. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472-478.
2. Finis D, Hayajneh J, König C, et al. Evaluation of an automated thermodynamic treatment (LipiFlow) system for meibomian gland dysfunction: a prospective, randomized, observer-masked trial. Ocul Surf. 2014;12(2):146-154.
3. Finis D, König C, Hayajneh J, et al. Implications of Meibomian Gland Atrophy on the Efficacy of Lipiflow treatment. Paper presented at: Association for Research in Vision and Ophthalmology (ARVO) 2014. May 4-8, 2014. Orlando, FL.
4. Baumann A, Cochener B. Meibomian gland dysfunction: a comparative study of modern treatments. J Fr Ophtalmol. 2014;37(4):303-312.
5. Qiao J, Yan X. Emerging treatment options for meibomian gland dysfunction. Clin Ophthalmol. 2013;7:1797-1803.
6. Dalton M. Conjunctivochalasis: An overlooked—but common—ailment. Eyeworld. Ocotber 2011. http://www.eyeworld.org/article-conjunctivochalasis. Accessed March 3, 2015.
Edward H. Jaccoma, MD
• specialist in laser and cataract surgery, dry eye, and aesthetic eye care at Associated Eyecare in Sanford, Maine
• director of New England Dry Eye, Kennebunk, Maine
• ejaccoma@aol.com
• financial disclosure: principal shareholder in eyeThera, a company specializing in dry eye care, and has received honoraria from TearScience
Andrew H. Jaccoma, MBA
• consultant at New England Dry Eye, Kennebunk, Maine
• vice president of sales and marketing at eyeThera
• andrew@eyethera.com

