
Over the last 2 decades, we have been gradually reinventing phacoemulsification. The first technological change that had a significant impact on my approach was torsional ultrasound with the INFINITI Vision System (Alcon), which really helped me rethink my procedure. Next, the CENTURION Vision System (Alcon) Active Fluidics allowed me to select and maintain IOP so I could define and plan precisely what I wanted to do in each procedure and carry out the plan safely and efficiently. Now the CENTURION Vision System with ACTIVE SENTRY Handpiece combines ACTIVE FLUIDICS (Alcon) technology with a pressure sensor in the handpiece that measures intraoperative IOP directly. Also available is a polymer-ended phaco tip, the INTREPID Hybrid Tip (Alcon), which is designed to reduce the risk of capsular tears. The combination has made my phacoemulsification procedure safer, plus more efficient and controlled than ever before.
Automated Fine Control of IOP
Before the CENTURION, operating at or near physiologic IOP was not safely feasible. When we got the CENTURION, the ability to operate at physiologic IOP was novel at first, but I found the transition to be very intuitive. It was certainly compelling because we are always trying to achieve normal visual physiological optics and normal physiologic pressure management in all disease states. Remaining at physiologic levels during surgery supports those goals.
With the introduction of the ACTIVE SENTRY Handpiece (Alcon), not only was it feasible to operate at or near physiologic IOP, but it also became possible to refine IOP to precise levels tailored to different patients. With ACTIVE SENTRY, continuous IOP monitoring, leakage compensation, and automated patient eye level (PEL) provide a noticeably more stable intraocular environment and mitigate instability that can arise. The handpiece gives me an even greater degree of subtlety, precision, and scalability. It allows me to approach any lens with a great deal of forethought and planning, thus helping ensure my confidence in the success of the procedure.
By offering precise control, the ACTIVE SENTRY Handpiece improves the safety profile of phacoemulsification. That new base line in safety advantage is enhanced tremendously with another remarkable innovation, the INTREPID Hybrid Tip.
The added Safety of Polymer Technology
Designed to lower the risk of damage to the capsular bag and other tissues, the INTREPID Hybrid Tip has a polymer end with no sharp or metal edges. The ultrasonic and fluidics performance are similar to the all-metal INTREPID Balanced Tip. Because of the decreased risk of capsular rupture with the Hybrid Tip, phacoemulsification can be performed closer to the capsule and/or with higher flow and vacuum levels. This can help surgeons operate more comfortably with their existing techniques and give them the confidence to evolve their procedures.
We always welcome ways to reduce the rate of capsule rupture to help in safer procedures with better outcomes. Used together, the ACTIVE SENTRY Handpiece and INTREPID Hybrid Tip are effective innovations I’ve seen in my career to decrease the incidence of capsule rupture.
I also use the INTREPID Transformer I/A Handpiece (Alcon), which has the same polymer technology. Using polymer-tipped instruments throughout the procedure gives a sense of ease to all steps of lens removal. I can focus more closely on the subtleties or complexities of procedures instead of focusing on the elements of risk. For example, during phacoemulsification, I’m less frequently trying to assess how close the instrument is to the capsule or iris. By changing my focus, I can look at broader aspects of the procedure, such as nucleus position, capsular stability, and fluidic dynamics. The all-polymer procedure feels like the wave of the future. It changes the way I interpret the procedure moment to moment, making it a richer, more fulfilling experience and a more efficient procedure overall.
Because the INTREPID Hybrid Tip enhances my ability to more confidently disassemble the nucleus with an increased safety profile, I choose to use it in all but the very densest of nuclei (up to grade 4). By marrying the ACTIVE SENTRY Handpiece and INTREPID Hybrid Tip, I get the greatest possible flexibility and versatility from the CENTURION Vision System platform.
Case: Safer, More Efficient Cataract Surgery
I performed cataract surgery on a 77-year-old woman with 2 to 3+ nuclear sclerosis and 2+ cortical changes.
A tapered sideport incision was made with a 1-mm blade. A square 2.2-mm clear corneal incision was made temporally. DisCoVisc OVD (Alcon) was used throughout the procedure. The approximately 5-mm capsulorhexis was decentered nasally 0.5 mm. Cortical hydrodissection was performed until the nucleus could spin freely within the capsular bag.
For phacoemulsification, I used the INTREPID Hybrid Tip, which has the familiar Balanced Tip design with an innovative polymer end. There are no metal edges on this tip, so at no point can metal contact the capsule or other intraocular structures (Figure 1). This makes the tip much less likely to cause damage to the capsule or iris. The performance of this tip is similar to its all-metal counterpart; it grooves very efficiently for divide and conquer, and it holds the nucleus well for a chopping technique.
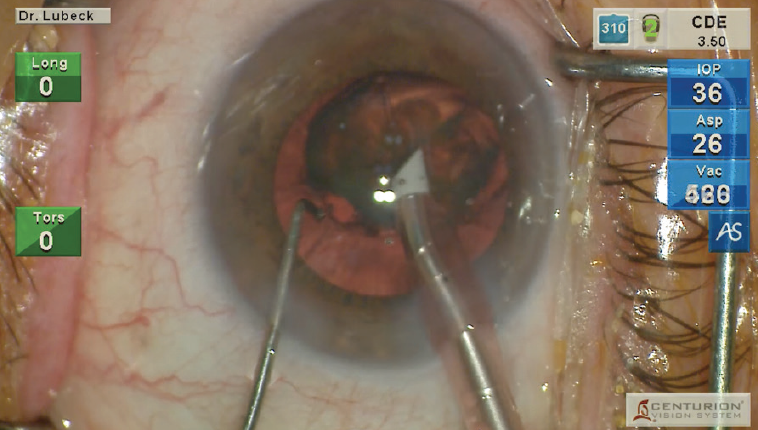
Figure 1. For phacoemulsification, I used the INTREPID Hybrid Tip, which has a familiar BALANCED design with an innovative polymer end. There are no metal edges on this tip, so at no point can metal contact the capsule or other intraocular structures.
ACTIVE SENTRY adjustments: Throughout the entire procedure, a sensor in the ACTIVE SENTRY Handpiece directly and continuously monitored IOP and managed the target IOP of 36. This technology also automates the patient eye-level function so that I do not need to sit the patient at any particular height to achieve the desired IOP for surgery.
The handpiece also adjusts for average incision leakage, making the chamber significantly more stable. This feature has allowed me to raise my aspiration and vacuum levels, permitting a more efficient and predictable nucleus disassembly and removal. In this case, ACTIVE SENTRY engaged 11 times during phacoemulsification. This means that, at 11 different moments, the technology prevented or mitigated a surge event (Figure 2). Whether you use the ACTIVE SENTRY Handpiece with the INTREPID Hybrid Tip or a standard balanced tip, it provides a significant procedural advantage over gravity-based systems that don’t have this level of sophistication in fluid management. I removed the nucleus using a CDE of 3.90, which appears to be lower than what I would have needed previously with a metal Balanced Tip and lower vacuum settings.
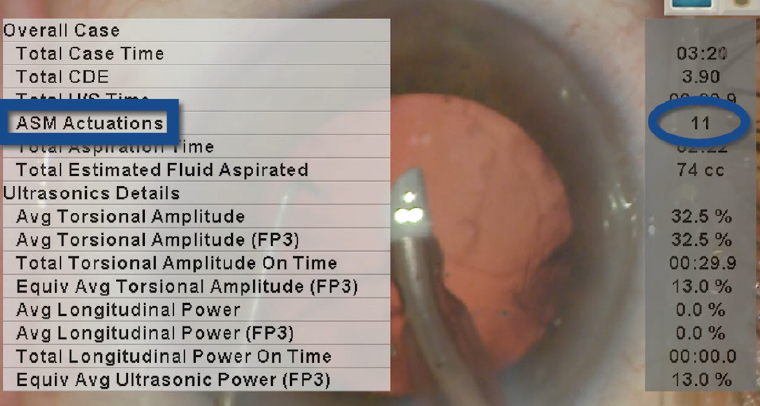
Figure 2. In this case, ACTIVE SENTRY engaged 11 times during phacoemulsification. This means that, at 11 different moments, the technology prevented or mitigated a surge event.
Cortex removal and polishing: Next, to remove the cortex, I used the INTREPID Transformer I/A Handpiece, which is also a novel and commendable innovation. In its primary mode, it is a coaxial polymer-tipped I/A handpiece. The polymer tip design allows me to place the tip up against the anterior and posterior capsules. When access to the subincisional cortex is required, the handpiece separates, and I insert the aspiration tip through the 1-mm sideport incision.
In this bimanual mode, I can easily assess the complete circumference of the capsular bag and polish the entire anterior capsule. If the capsule is at all unstable, then the bimanual mode facilitates easier cortex removal. When posterior capsular polishing is needed, the capsule can be drawn into the aspiration port and the tip passed across the capsular plane, yielding the clearest possible capsule.
Finally, I inserted the new lens. The viscoelastic was aspirated from the anterior chamber and behind the lens, finishing the cataract surgery.
Case: A Smooth Process with an Intraoperative Adjustment
Using the LENSX femtosecond laser (Alcon) I performed surgery on a 72-year-old woman with a 2 to 3+ nuclear and 2+ cortical cataract.
After opening the incisions, the capsule was drawn centrally to make sure that it was free and had no microadhesions. Hydrodissection was performed gently and slowly until all gas had been released anteriorly and the nucleus could be rotated within the capsular bag. Phacoemulsification was performed using the ACTIVE SENTRY Handpiece for fluidics management and the INTREPID Hybrid Tip, a balance-designed tip with a polymer end. The polymer tip’s efficiency is similar to a metal balanced tip, so it engages the nucleus and holds easily for division and emulsification of individual segments.
Maintaining target IOP with ACTIVE SENTRY: The ACTIVE SENTRY IOP Handpiece sensor continually, directly monitors IOP throughout the procedure, communicating with ACTIVE FLUIDICS. The system automates patient eye level, so it’s no longer necessary to set that on the panel or position the patient at a certain height. It also adjusts for average leakage from incisions. All of this occurs automatically in the background, engaging intermittently as needed to mitigate surge events and maintain chamber stability.
In this case, where the lens is graded a 2 to 3+, it was emulsified very efficiently. ACTIVE SENTRY allowed me to increase the flow and vacuum rates by as much as 30% and maintain a very stable chamber, even working at a near-physiologic IOP of 36 mm Hg (Figure 3).
The polymer Hybrid Balanced Tip is exceptionally capsule-friendly, allowing me to work much closer to the capsule for nucleus, epinucleus, and even partial cortex removal. Many of the maneuvers I performed would not be feasible with a metal balanced tip.
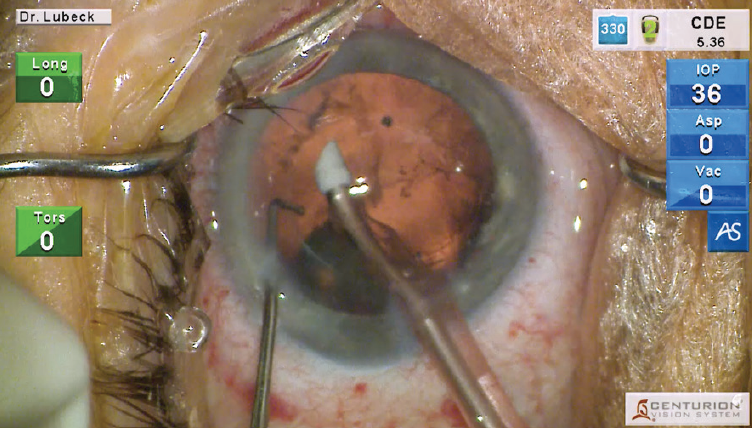
Figure 3. The grade 2 to 3+ nucleus was emulsified efficiently. ACTIVE SENTRY allowed the flow and vacuum levels to be raised by as much as 30% and maintain a stable chamber while operating at a near-physiologic IOP of 36 mm Hg.
Phacoemulsification required a CDE of 5.89. The ACTIVE SENTRY engaged a total of seven times during nucleus removal.
Cortex removal and polishing: Irrigation and aspiration of the cortex were done with the INTREPID Transformer I/A Handpiece, another Alcon polymer-tipped aspiration instrument (Figure 4). This handpiece starts as a coaxial I/A and converts to a bimanual if needed. The second handpiece is disengaged from the back of the first, and the aspiration tip is inserted through the 1-mm sideport incision. It can be used to polish the posterior capsule and remove any cortex that was inaccessible with the handpiece in coaxial mode. The aspiration port on the transformer bimanual handpiece has an oval contour that’s ideal for polishing the capsule. For the posterior capsule, polishing can be achieved by gently engaging the capsule with the tip and then dragging the tip slowly across the capsular surface.
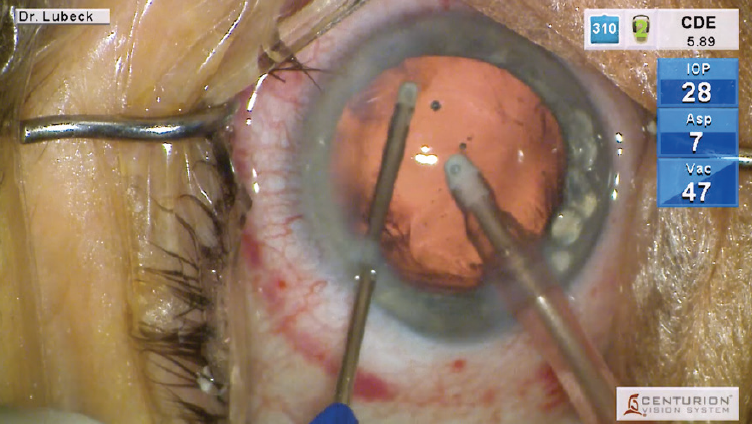
Figure 4. The cortex was irrigated and aspirated with the INTREPID Transformer I/A handpiece, the polymer-tipped instrumentation for cortex removal and capsule polishing.
Intraoperative aberrometry and lens implantation: The anterior chamber and capsular bag were filled with ProVisc OVD (Alcon) and the pressure raised to the appropriate level. I turned off the microscope light, and the patient fixated on the red light within the ORA SYSTEM technology (Alcon) so I could take several series of measurements. A lens was chosen and implanted to provide the desired outcome.
Once again, I used the INTREPID Transformer I/A Handpiece for aspiration of the viscoelastic. The polymer tip is ideally designed to go behind the lens and safely work close to the capsule. It’s also an excellent lens manipulator, so it can be used to center and rotate the IOL.
The combination of the ACTIVE SENTRY Handpiece and ACTIVE FLUIDICS, with the polymer technology of the INTREPID Hybrid Tip and INTREPID Transformer I/A Handpiece, results in a very efficient and improved procedure. With precise control of IOP throughout surgery and lower risk of injury from the polymer-tipped instruments, I can focus on surgery with less concern about inducing complications.



