IOL Exchange: Advantages, Disadvantages, and Alternatives

Advances in cataract surgery and IOL technology have dramatically improved surgical outcomes and decreased perioperative complications. Nevertheless, situations arise that require repositioning, exchange, or removal of a previously implanted lens.
RATES OF EXCHANGE
Over time, the rate of IOL exchange has declined. It was 1.75% in a review of cases from 1986 to 1990,1 0.77% in a later study (cases from 1998-2004),2 and 0.53% in a more recent report (cases from 2007-2011).3 As cataract surgery has evolved, so have the indications for IOL explantation or exchange. Originally, most explanted lenses were anterior chamber IOLs, and their removal was usually due to pseudophakic bullous keratopathy, uveitis-glaucoma-hyphema syndrome, or cystoid macular edema.4 Since posterior chamber IOLs (PCIOLs) became preferred, the main indications for explantation or exchange have become IOL dislocation or decentration, refractive concerns such as incorrect lens power, subjective visual symptoms, and opacification of the optic.3
The shift in indications from ocular morbidity to patients' dissatisfaction may dissuade cataract surgeons from explantation; the associated intraoperative risks and postoperative complications may outweigh the frustrations of an otherwise healthy patient. Furthermore, insurance coverage can be difficult to obtain unless surgery is deemed medically necessary. For these reasons, the published rates of IOL exchange may underestimate the number of patients who could benefit from such a procedure.
INDICATIONS
Almost half of IOL exchanges are attributable to either incorrect IOL power or patients' dissatisfaction for reasons such as dysphotopsia.3 Despite advances in biometric and topographic analysis, refractive outcomes are still imprecise. In a study of more than 17,000 cataract surgeries in Sweden, only 55% of eyes achieved planned emmetropia (defined as a spherical equivalent of ±0.50 D from plano and < 1.00 D of astigmatism).5 Simon et al recently published their experience at a teaching institution: although 67% of patients were within ±0.50 D of the targeted refraction postoperatively, fully one-third had a residual refractive error that was more than 0.50 D than intended.6
Patients are undergoing cataract surgery at a younger age7 and have higher expectations with regard to postoperative vision than in the past. Today, a lot of patients desire at least partial spectacle independence. Despite achieving what many people would consider excellent postoperative Snellen visual acuity, patients may seek an IOL exchange due to subjective visual concerns, including reduced contrast sensitivity, glare, halos, and flashes.8,9 Dysphotopsias are a leading cause of patients' dissatisfaction after cataract surgery, but a large proportion tolerate these visual phenomena because few options for treatment pose minimal risk. Hypothetically, more patients would desire—and more surgeons would be comfortable with—IOL exchange, were it not for the risks and technical challenges of the lens' removal.
Pseudophakic children are a unique group that might also benefit from innovations in IOL exchange techniques. In one study of this population, 99 of 114 eyes (86.8%) had a myopic shift in refraction, with the majority experiencing a change of up to 0.50 D per year.10 The timing of IOL exchange and ideal target refraction in pseudophakic children are unclear, but a lower risk profile for the procedure could significantly alter practice patterns.
RISKS
Visual outcomes after IOL exchange can be excellent, but again, surgery carries many risks. Anterior vitrectomy is the most common intraoperative complication, noted in up to 85% of PCIOL explantations.11 A more recent study reported a lower rate of 33.3%, but that number is not insignificant.3 The risk is greater in patients with an open posterior capsule such as those who have undergone an Nd:YAG posterior laser capsulotomy.12 Another common complication is zonular dehiscence, noted in up to 44% of IOL exchanges.13
To remove a PCIOL from the capsular bag, most surgeons use intraocular scissors to fragment the IOL and then remove the pieces. In order to prevent trauma to the zonules, some ophthalmologists remove only the optic and leave behind the haptics, because they may be adherent to the capsular bag.14 These haptics, however, can dislocate into the optical axis or vitreous, or they can interfere with the position of the new IOL. Surgery to reposition or exchange an IOL that has dislocated into the vitreous cavity requires concurrent pars plana vitrectomy and carries numerous risks, including postoperative cystoid macular edema and retinal detachment.15
It is generally preferable to implant the replacement IOL in the capsular bag. If this is not possible, the new IOL can be placed in the sulcus or anterior chamber. Scleral fixation of a PCIOL is also possible. It carries the risk of suture rupture with subsequent IOL dislocation, retinal detachment, and ocular hypertension, however, and is associated with a high rate of additional surgery.16 Although less common with modern designs, there are still complications related to the placement of an anterior chamber IOL such as pseudophakic bullous keratopathy.17
ALTERNATIVES
Rather than subject a patient to the risks of a full IOL exchange, some surgeons implant a second (piggyback) IOL anterior to the original. This procedure can be technically difficult and carries unique risks. For instance, intralenticular opacification can develop, as cells proliferate in the interface between the IOLs.18-20 Although this complication can be treated with the Nd:YAG laser,21 doing so carries a risk of damage to the lenses or a shift in the IOLs' positions that alters refraction. A piggyback IOL can also be placed in the sulcus, but the lens may then cause pigment dispersion from iris chafing, leading to sustained ocular hypertension and secondary pigmentary glaucoma.22,23 It has also been noted that, although a rare occurrence, a piggyback IOL can shift, resulting in postoperative pupillary optic capture.24
LASIK and PRK have both been used to correct residual refractive error after cataract surgery. Although these procedures avoid the risks of a second intraocular operation, their results are not as good as generally reported for initial laser refractive surgery.25 In one study, less than half of pseudophakic patients undergoing laser refractive surgery had a UCVA of 20/20 or better postoperatively.25 The reasons for this difference are unclear but may be related to patients' age, corneal decompensation, or the higher likelihood of ocular comorbidities in this population.
FUTURE DIRECTIONS
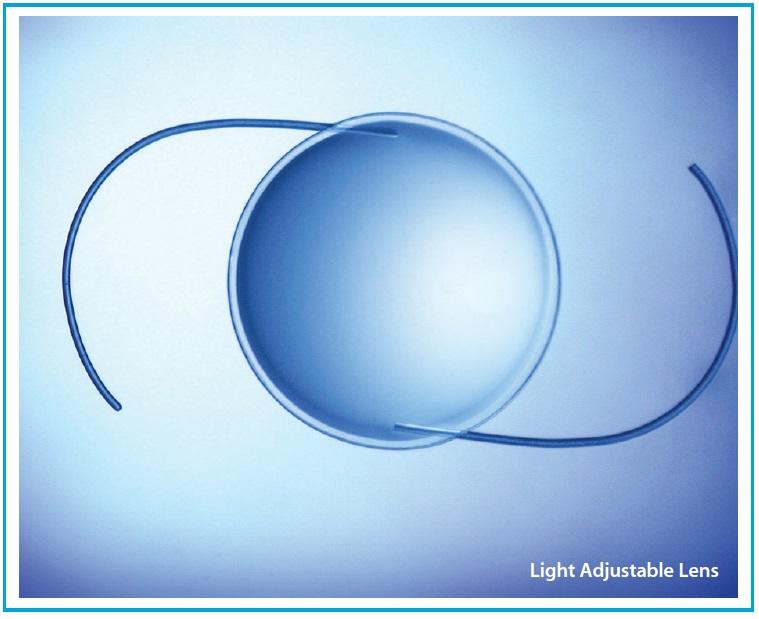
Technologies in development to improve refractive outcomes after cataract surgery could alter the need for some IOL exchanges. Postoperatively, the power of the Light Adjustable Lens (LAL; CalhounVision) can be adjusted by a “lock-in” treatment with ultraviolet (UV) light. In one study, use of an LAL led to a final refraction within 0.50 D of target in 97% of eyes.26 Although these numbers are impressive, the LAL may have some drawbacks. After surgery but prior to the lock-in treatment, patients need to wear dark sunglasses to protect their eyes from any external source of UV light. Adherence is a well-known problem in medical therapy and could be an issue with the LAL as well. After the lock-in procedure, there is currently no option to further modify the refractive power of the LAL. This means that a change in the patient's refraction, astigmatism, or visual needs after the final UV light treatment would still necessitate a traditional IOL exchange.
Also in development is the Harmoni Modular IOL (ClarVista Medical).27 This IOL is being developed to facilitate atraumatic lens exchange when needed by isolating optic fixation from capsular bag fixation. The separation reportedly allows the optic to be exchanged without manipulation of the capsular bag, while also providing novel solutions for addressing posterior capsular opacification and effective lens position at the time of the lens' initial implantation.
The development of IOLs that can be modified by femtosecond lasers is also being explored, but these technologies are unproven and years away from clinical trials.28
CONCLUSION
The US population is aging. An estimated 30 million people in this country will have cataracts by the year 2020, with the total number of cataract surgeries each year in the millions.29 Complications that affect even a small percentage of patients will therefore occur in significant numbers. An IOL exchange rate of 0.5% equates to 5,000 per 1 million cataract surgeries. With current techniques, thousands of patients annually would therefore experience the intraoperative and postoperative complications discussed herein, with the accompanying risks and costs of additional medical treatments, further surgery, and associated vision loss. New technologies that minimize the need for an IOL exchange or that make the procedure technically easier to perform would theoretically reduce these risks significantly, offer patients more options, improve outcomes, and decrease health care expenses. n
Anna Lehmann
• medical student, Baylor College of Medicine, Houston
• alehmann@bcm.edu
• financial disclosure: none acknowledged
Jeffrey R. SooHoo, MD
• assistant professor of ophthalmology, University of Colorado Eye Center, Aurora
• jeffrey.soohoo@ucdenver.edu
• financial disclosure: none acknowledged
Ready to Claim Your Credits?
You have attempts to pass this post-test. Take your time and review carefully before submitting.
Good luck!
Recommended
- General
Art and Science Inside and Outside the Clinic
Ben Lahood, MD, MBChB(dist), PGDipOphth(dist), FRANZCOBen Lahood, MD, MBChB(dist), PGDipOphth(dist), FRANZCO

