
Sponsored By


Over the years, cataract surgeons have become increasingly focused on the refractive accuracy of our surgical results. This is in part due to the high patient demands of today, but also in part because of the sophisticated technologies we now have available to help us achieve such excellent results. One of the challenges that we still face, however, is meeting our patients’ expectations with the abundance of IOL technologies available to them. In other words, with a plethora of IOLs to choose from, how can we refine our selection in order to provide patients with the individualized, high-quality vision they desire?
INCREASING DEMAND, REFRACTIVE NEEDS
It is true that patient demand for premium lens technologies has increased, and with it has come an increase in their refractive needs. This is especially true in patients who present with enough astigmatism to benefit from a toric IOL. It has been shown that, in nearly one-third of eyes, moderate to high astigmatism (>1.00 D) is present.1 The benefits of a toric IOL extend beyond this range, and today I may also implant toric IOLs in patients with as little as 0.50 to 0.75 D of anterior keratometric astigmatism (ie, against-the-rule astigmatism).
There are several factors that can affect the refractive accuracy of a toric IOL:
1. Just 10º of misalignment can cause a decrease in the desired refractive effect of up to 33%;2
2. Manual reference axis and toric axis marking can contribute to a mean total error in toric IOL alignment of 4.9 ±2.1º;3 and
3. Without intraoperative automated assistance in alignment of the toric IOL, only 60% of patients will exhibit postoperative results within ±0.50 D of the intended refraction.4
Luckily for cataract surgeons, we have a variety of devices available to aid in refining our outcomes with all types of IOLs, including toric IOLs. These include but are not limited to the IOLMaster 500 and 700 (Carl Zeiss Meditec), Lenstar (Haag-Streit), Pentacam, (Oculus), Aladdin (Topcon), Galilei G6 (Ziemer), ORA System With VerifEye Technology (Alcon), iTrace (Tracey Technologies), Cassini Corneal Shape Analyzer (i-Optics), and OPD-Scan III (Nidek). In my experience, the most advantageous technology that has allowed me to more successfully meet the refractive needs of my astigmatism patients and, in addition, improve my workflow, is the IOLMaster 700. This is an integral component of the ZEISS Cataract Suite, a line of products intended to work together for markerless toric IOL alignment.
ADVANTAGES OF THE IOLMASTER 700 AND CALLISTO eye
The IOLMaster has long been the gold standard in biometry. The latest iteration, the IOLMaster 700 (Figure 1A), uses swept-source OCT imaging with fixation check (Figure 1B). In addition to the B-scan measurements of central corneal thickness, anterior chamber depth, lens thickness, and axial length, it also performs automated keratometry with distance-independent telecentrics technology, horizontal white-to-white, and pupil offset measurements (Figure 2). Additionally, as it is taking these measurements, the CALLISTO eye (Carl Zeiss Meditec) simultaneously captures a reference image, identifying landmarks on the surface of the eye. These landmarks, which correspond with the keratometry reading of the IOLMaster 700, can aid in toric IOL alignment. When using this technology, the percentage of patients who will be within ±0.50 D of the intended refraction is much higher than the 60% who achieve that level of refractive accuracy when no intraoperative assistance is used.
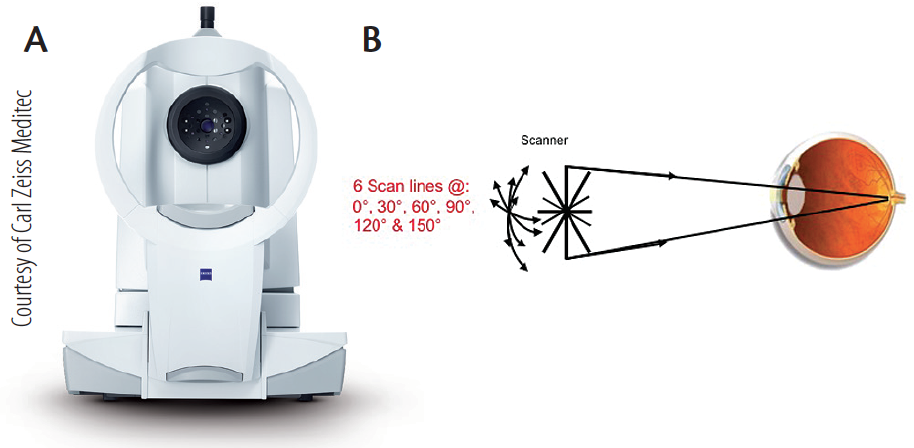
Figure 1. The IOLMaster 700 (A) incorporates swept-source OCT imaging with fixation check (B).
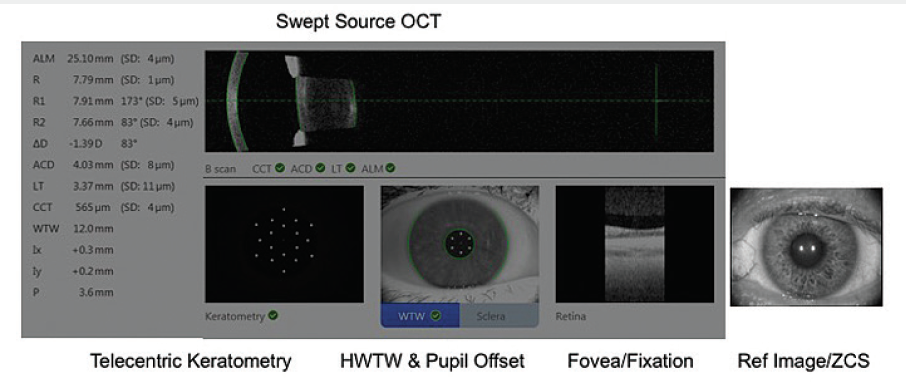
Figure 2. Measurements taken with the swept-source OCT function of the IOLMaster 700.
What I like about the swept-source OCT function of the IOLMaster 700 is that I can take a full-length scan of the entire eye. Not only can I visually verify measurements, but I can also detect unusual eye geometries. Furthermore, the risk of refractive surprises is reduced thanks to my ability to visualize the foveal pit with the fixation check software.
The other potential benefit of the machine includes the prediction of the effective lens position (Figure 3). I measure all of my patients postoperatively because, although we have many toric lenses to choose from, there is currently none available to correct down to less than 0.50 D keratometric cylinder. In these cases, I will consider using limbal relaxing incisions (LRIs) to treat the astigmatism. I also use the IOLMaster 700 in these eyes, too. When I re-measure their keratometry postoperatively with the device, I am still able to see the lens.
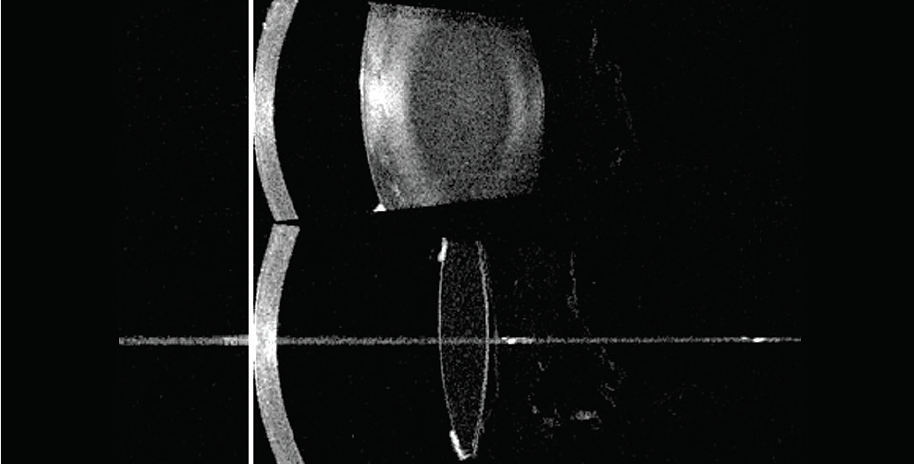
Figure 3. Effective lens position prediction is possible with the IOLMaster 700.
CASE PRESENTATION
In addition to the benefits of the IOLMaster 700 in conjunction with the CALLISTO eye for toric IOL alignment, the device has many other clinical benefits in routine cataract surgery. Below is one example.
A 53-year-old female presented to my clinic with decreased vision, glare, and difficulty driving at night for more than 1 year. Upon examination, it was noted that the visual acuity in her right and left eyes, respectively, was 20/200 and counting fingers. In her right eye, there was a grade 2+ nuclear sclerotic and grade 3+ posterior subcapsular cataract; in her left eye, she had a grade 2 to 3+ nuclear sclerotic and grade 3 to 4+ posterior subcapsular cataract (Figure 4). The lens was also slightly tilted on axis compared to the visual axis of the patient.
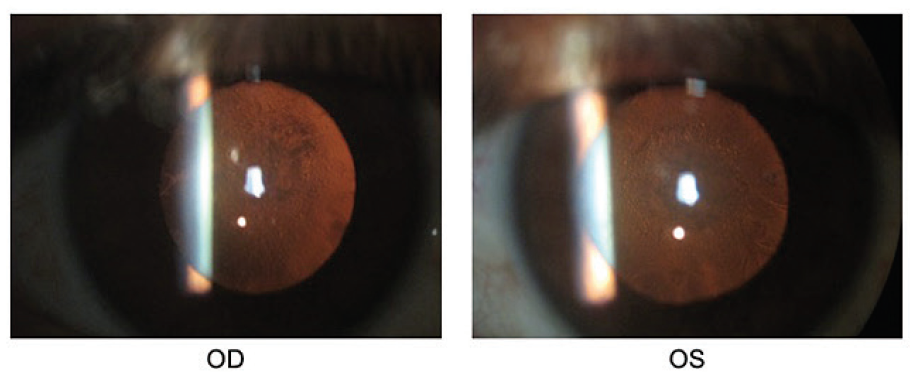
Figure 4. Presentation of the patient’s right and left eyes preoperatively.
In this case, measuring the eye with an optical interferometry device would be limited by the opacity of the cataract.
The risk with using an automated keratometry device for this and all cases is that, because it measures the distance between the first Purkinje reflections, it is a variable technique. With the IOLMaster 700, however, I can use the telecentric keratometry function to produce accurate and reproducible K readings. This device creates distance-independent spacing of the first Purkinje reflections, so it allows the points to remain in the same distance from each other, even if the instrument moves or if the tear film varies. Additionally, the IOLMaster 700 facilitates a faster measurement than other devices, captures prior to destabilization of the tear film, and contributes to an enhanced patient workflow.
CONCLUSION
The IOLMaster 700 is just one dynamic component of the ZEISS Cataract Suite. Combining its use with the CALLISTO eye for the alignment of toric IOLs has increased the refractive results of my patients and put more people into the zone of being within ±0.50 D of the intended correction.
Using the technologies in the ZEISS Cataract Suite has not only improved the workflow of my practice, it has also built my confidence in my ability to get the measurements that I need in every case, whether in astigmatism correction or standard cataract surgery. Also, it has resulted in significant expansion of my special design lens implantation percetage. I have the peace of mind that, when I take measurements to the operating room, I will obtain the postoperative results that I had intended and that my patients had hoped for. n
1. Hoffmann PC, Hütz WW. J Cataract Refract Surg. 2010;36(9):1479-1485.
2. Visser N, Berendschot TT, Bauer NJ, et al. Accuracy of toric intraocular lens implantation in cataract and refractive surgery. J Cataract Refract Surg. 2011;37(8):1394-1402.
3. Miyake T, Kamiya K, Amano R, et al. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1653-1660.
4. Behndig A, Montan P, Stenevi U, Kugelberg M, et al. Aiming for emmetropia after cataract surgery: Swedish National Cataract Registry. J Cataract Refract Surg. 2012;38(7):1181-1186.
The statements of the healthcare professionals giving this presentation reflect only their personal opinions and experiences and do not necessarily reflect the opinions of any institution with whom they are affiliated.
The healthcare professionals giving the presentation may have a contractual relationship with Carl Zeiss Meditec, Inc., and may have received financial compensation.