CASE PRESENTATION
A 45-year-old man presents for a refractive surgery consultation. The patient’s current medical regimen consists of icosapent ethyl 2 g by mouth twice daily for the treatment of hypertriglyceridemia and lisinopril 10 mg by mouth once daily for the treatment of hypertension. His surgical history is significant for the removal of a nasal tumor from the right sinus.
The patient’s BCVA is 20/20 OU with a manifest refraction of -4.25 +1.00 x 157º OD and -3.00 +0.25 x 035º OS. The findings of a slit-lamp examination are normal in each eye with no staining. Schirmer testing is 14 mm OD and 12 mm OS with anesthesia. Corneal sensation is depressed in the right eye and normal in the left eye (Figure 1). The patient reports no history of dry eye disease (DED) or DED treatment. He has a history of successful contact lens wear with a mild defocus of -0.50 D OD for near and full correction in the left eye for distance.

Figure 1. The corneal displays for the right (A) and left (B) eyes have a normal appearance.
After a discussion, the patient elects to undergo bilateral laser vision correction (LVC) with an undercorrection of -0.50 D in the right eye and full correction in the left eye. Uneventful LASIK surgery using the WaveLight EX500 with Contoura Vision (Alcon) is performed. The flap is created with the WaveLight FS200 femtosecond laser (Alcon).
One day after surgery, the patient’s UCVA is 20/400 OD and 20/25 OS. A manifest refraction produces no improvement in the left eye. Grade +4 and +1 superficial keratopathy is detected in the right and left eyes, respectively. The flap in the left eye is well positioned. Visually significant microstriae and a displaced LASIK flap are observed in the right eye. The right flap is relifted and refloated without incident, and a bandage contact lens is placed. Occlusion of the lower puncta with silicone plugs is performed.
On postoperative day 2, the bandage contact lens is removed. The patient’s UCVA is 20/40 OD, 20/40 OS, and 20/20+1 OU. Photobiomodulation with low-level light therapy (Espansione-Red 633 nm, Espansione Group) is performed. Perfluorohexyloctane ophthalmic solution (Miebo, Bausch + Lomb) instilled bilaterally three times per day is added to his drug regimen of difluprednate ophthalmic emulsion 0.05% (Durezol, Alcon) and gatifloxacin ophthalmic solution 0.3% (Zymar, AbbVie), both administered three times per day in each eye.
On postoperative day 4, grade +3 to +4 and grade +1 to +2 lissamine green staining is observed in the right and left eyes, respectively. The patient’s UCVA is 20/60 OD, 20/30 OS, and 20/30 OU, with no improvement on manifest refraction.
When the patient returns 7 days after LASIK surgery, his UCVA is 20/400 OD and 20/20-2 OS, with no improvement on manifest refraction. He reports blurry vision, a burning sensation, and pain in the right eye. Confluent superficial punctate keratitis is observed in the right eye, and grade +1 to +2 superficial punctate keratitis is found in the left eye. The tear breakup time (TBUT) without anesthesia is 1 second in the right eye and 7 seconds in the left eye.
How would you proceed?
—Case prepared by Karl G. Stonecipher, MD, and Adrianna Bevis, BS

KENNETH BECKMAN, MD, FACS
Severe ocular surface disease is the cause of the patient’s poor vision and is complicated by a lack of corneal sensation. He was found to have normal tear production and neurotrophic corneas preoperatively, and the latter are typically aggravated by LASIK.
The DED must be managed. Treatment with preservative-free artificial tears—to limit potential toxicity—and whichever prescription DED medication his insurance plan covers would be initiated. Therapy with a topical steroid might also be beneficial. If the patient is unresponsive to conventional prescription DED therapy, an amniotic membrane graft and autologous serum would be the next steps.
If corneal healing is not observed with the aforementioned methods, cenegermin-bkbj ophthalmic solution 0.002% (Oxervate, Dompé) would be prescribed to treat the neurotrophic keratitis (NK). It might take several weeks for the patient’s insurance company to approve coverage of this medication. Aggressive DED therapy would be continued in the interim. Even after the ocular surface heals, he will likely need long-term DED therapy to limit recurrences.

BRENT KRAMER, MD
Sometimes, simple interventions—ensuring adequate hydration, reducing environmental stressors such as ceiling fan use at night, and optimizing basic lid hygiene—can have a surprisingly big impact on short-term ocular dryness during the early postoperative period after LASIK. The markedly reduced TBUT in the patient’s right eye, however, suggests significant meibomian gland dysfunction.
Broadband light or intense pulsed light therapy with manual gland expression would be performed every 2 weeks for four sessions, at which point the patient would be reassessed. Addressing the evaporative component of DED would be critical to restoring tear film stability and improving his ocular comfort. Perfluorohexyloctane ophthalmic solution has become a staple in my treatment of ocular dryness related to meibomian gland dysfunction, so it is reassuring to see that treatment with this drug was started early in the postoperative period.
The patient’s decreased corneal sensation before LVC raises suspicion of subclinical NK that manifested after LASIK. The reduced sensation could be secondary to trigeminal nerve damage from the prior tumor resection. In situations like this, a cryopreserved amniotic membrane and platelet-rich plasma tears are often my first step toward supporting epithelial healing and reducing inflammation. They are temporizing measures. Once a diagnosis of NK is reached, I immediately initiate the process to obtain cenegermin-bkbj for corneal nerve regeneration. The drug remains the only US FDA-approved treatment for NK and has revolutionized the management of this challenging condition. As drug development advances, I anticipate broader use of recombinant human nerve growth factor after ocular surgery—not only to treat but potentially to prevent short-term ocular dryness and neuropathic pain.

SHERI ROWEN, MD, FACS
Situations like this one are unfortunately all too common. An excellent preoperative assessment uncovered a warning sign: depressed corneal sensitivity. I wish all patients underwent similar testing before proceeding to refractive corneal surgery.
The patient had no other signs of DED, staining, or contact lens intolerance. Not realizing there might be an issue, the surgeon performed LASIK. The displaced flap was a confounding incident.
During the early postoperative period, both eyes exhibited signs of dryness, significant fluorescein staining, and highly significant lissamine green staining. All of these could be attributed to severe DED alone, but my working diagnosis would be NK. I would immediately initiate the process to obtain cenegermin-bkbj. While awaiting insurance approval, I would initiate treatment with a cryopreserved amniotic membrane graft (AmnioGraft, BioTissue) in the right eye to provide much-needed trophic factors.
I had a similar case in 2022. A 68-year-old woman presented to my practice for a consultation. The patient had undergone cataract surgery with an extended depth of focus IOL (AcrySof Vivity, Alcon) in the right eye and a toric IOL in the left eye. She worked as a hair stylist and could not see well enough to function without glasses. She desired improved near visual acuity.
An initial examination revealed mild corneal staining bilaterally. Punctal plugs were inserted in the lower puncta, and therapy with lifitegrast ophthalmic solution 5% (Xiidra, Bausch + Lomb) was initiated. One month later, the staining had resolved, and the TBUT had improved. A monovision contact lens trial was successful. The following month, the patient underwent LASIK with the Femto LDV (Ziemer Ophthalmic Systems) and WaveLight EX500 excimer laser.
One day after surgery, the patient described an uncomfortable pricking sensation in her eyes that worsened over the following days. Her vision subsequently decreased significantly, and she reported significant pain. Three weeks after surgery, a band of staining was visible in the hot zone, just below the pupil—typical of NK—and corneal sensation had decreased. Topography obtained that day was frightening and suggested a decentered LASIK ablation (Figure 2). Based on these findings, the patient’s age, and her history, I began the process to obtain cenegermin-bkbj.
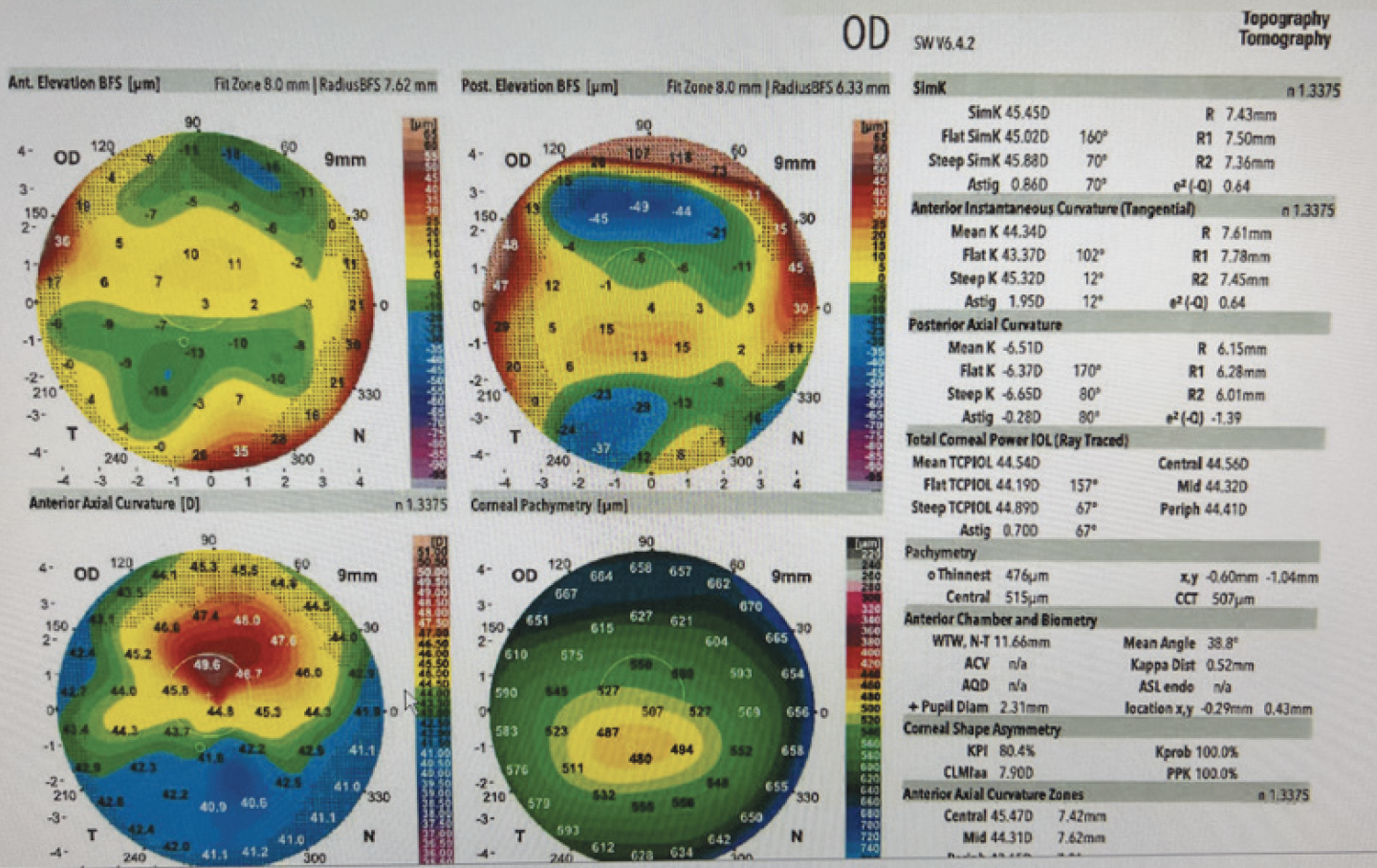
Figure 2. Topographic maps for one of Dr. Rowen’s patients 3 weeks after bilateral LASIK surgery.
Figures 2 and 3 courtesy of Sheri Rowen, MD
After 3 weeks of treatment, the patient returned with perfect vision and no pain. Topography showed a well-centered ablation (Figure 3). I was amazed that the topographic findings had been so abnormal during the acute phase.

Figure 3. Topography of the same eye shown in Figure 2 after 3 weeks of treatment with cenegermin-bkbj.
NK is a great masquerader, and proper diagnosis and treatment are the ophthalmologist’s responsibility. I firmly believe that corneal sensation testing should be a routine part of the preoperative evaluation for LVC and that ophthalmologists should maintain a high index of suspicion for NK if corneal sensation is reduced and central to inferior central staining is present after ocular surgery. DED must be treated as well. Clinicians often think only of DED when evaluating patients like these, but DED is on the spectrum of neurotrophic disease.


WHAT WE DID: KARL G. STONECIPHER, MD, AND ADRIANNA BEVIS, BS
Five days after surgery, the upper puncta were occluded with silicone plugs, and low-level light photobiomodulation was repeated. Treatment with cenegermin-bkbj ophthalmic solution 0.002% was initiated for the NK, which was more severe in the right than in the left eye.
The operative notes for the patient’s tumor removal were requested. A review of the notes revealed that the nasolacrimal system on the right side had been removed with an unspecified amount of irradiation over the course of 1 month at divided intervals.
One month after LASIK surgery, the patient’s UCVA was 20/25-1 OD and 20/20 OS. His BCVA was 20/20-2 with a manifest refraction of +0.25 +0.25 x 120º OD and 20/20+1 with a plano refraction OS. The TBUT was 5 seconds in the right eye and 7 seconds in the left eye. Fluorescein staining was +1 in the right eye and +1 to +2 in the left eye (Figure 4).

Figure 4. The UCVA and staining markedly improved in the patient’s right (A) and left (B) eyes, but significant inferior staining persisted.
Figure 4 courtesy of courtesy of Karl G. Stonecipher, MD
An evaluation of corneal sensation before LVC is not routine practice but can provide useful information. Cenegermin can be extremely effective for the treatment of severe DED, but intervention must be initiated early.