KEY TAKEAWAYS
- Fibrosed capsular bags can make late IOL exchange high risk after refractive surprises, premium IOL dissatisfaction, ACCS-induced decentration, or macular disease
- The fixOflex endocapsular device separates the IOL from capsular tissue to preserve bag architecture and keep IOL exchange surgically feasible
- Early cases showed greater capsular clarity, stable IOL position at 6 months, and manageable IOL exchange after late age-related macular degeneration

Recent advances in cataract surgery have substantially increased its safety and predictability, but refractive surprises, dysphotopsias with presbyopia-correcting IOLs, IOL decentration secondary to anterior capsular contraction syndrome (ACCS), and late IOL incompatibility caused by macular disease can still occur. These clinically distinct problems share a common limitation: once the capsular bag has fibrosed and fused with the IOL, meaningful intervention is often difficult. Devices such as the fixOflex (FOF; EyePCR), which received the CE Mark in February, are designed to address this limitation by preserving the endocapsular bag.1
THE CLINICAL PROBLEM
Refractive Surprises and the Limits of Prediction
Despite advances in optical biometry and IOL power calculation formulas, refractive surprises can occur after cataract surgery. Eyes with a history of corneal refractive surgery, extreme axial length, or irregular astigmatism are particularly susceptible to calculation errors. Further, even when the immediate postoperative refraction is on target, long-term stability cannot be guaranteed. Changes in axial length, zonular relaxation, and subtle shifts in the effective lens position can produce a clinically meaningful refractive drift over time.
In conventional cataract surgery, IOL exchange is generally feasible only during the early postoperative period, while the capsular bag remains pliable and accessible. Beyond that window, adhesion between the IOL optic and the posterior capsule, combined with anterior capsular fibrosis, generally renders an IOL exchange a high-risk procedure with a poor benefit-to-risk ratio. In eyes with a mature, fibrosed capsular bag, the procedure is rarely attempted.
Dissatisfaction With Presbyopia-Correcting IOLs
Premium IOLs—including bifocal, extended depth of focus, and trifocal designs—are associated with patient dissatisfaction attributable to glare, halos, reduced contrast sensitivity, and a mismatch between preoperative expectations and postoperative visual experience. Most patients’ level of satisfaction improves over time through neural adaptation or spectacle correction. For those who remain dissatisfied, an IOL exchange or supplementary lens implantation may offer the most effective path to resolution. Capsular fibrosis, however, closes the surgical window long before many of these patients reach a definitive decision.
IOL Decentration and Tilt From ACCS
ACCS receives considerably less clinical attention than posterior capsular opacification, yet the former is an important complication. Mild anterior capsular phimosis is common and often asymptomatic; however, asymmetric contraction can induce clinically significant IOL displacement. Eyes with pseudoexfoliation syndrome, uveitis, or myotonic dystrophy are at elevated risk.
The optical performance of premium IOLs depends on precise centration. The performance of rotationally asymmetric designs, segmented bifocal optics, and toric lenses can be substantially degraded from even minor decentration or tilt. Treatment options are limited to observation; Nd:YAG laser anterior capsulotomy, which may further destabilize the lens; and high-risk surgical revision.
In everyday clinical practice, a patient may have excellent IOL centration immediately after surgery and return several months later with clear IOL decentration. In this situation, surgeons often have little practical recourse beyond observation.
Late Macular Pathology and IOL Incompatibility
An underappreciated but clinically important scenario is the development or progression of macular disease following premium IOL implantation. Multifocal and extended depth of focus optics perform optimally in eyes with a healthy macula; optical compromises such as light splitting and contrast reduction are offset by the benefit of an extended focal range. When age-related macular degeneration, epiretinal membrane, or macular edema supervenes, however, these lenses can become a liability. Their light-distributing properties may further compromise the residual central vision on which the patient most depends, and the benefits of multifocality are largely lost.
Historically, surgeons and patients in this situation have had few options. The explantation of an IOL from a fibrosed capsular bag complex carries substantial risks—including zonular dehiscence, vitreous prolapse, and corneal endothelial damage—and is typically judged to carry more risk than benefit.
A PROACTIVE SOLUTION
By establishing a stable, biocompatible chamber that preserves capsular architecture and maintains long-term IOL exchangeability, the FOF may make the aforementioned clinical problems more manageable.2
The FOF is implanted within the capsular bag at the time of cataract surgery.1 This foldable, biocompatible endocapsular device houses the IOL within an inner chamber while physically separating the IOL optic from the capsular epithelium. This separation is intended to inhibit the migration and proliferation of lens epithelial cells—the cellular substrate of both posterior capsular opacification and ACCS. The critical functional property of the FOF is that the IOL retained within the device’s chamber remains retrievable and exchangeable after the primary procedure without direct adhesion to capsular tissue.
The FOF and similar devices in development for endocapsular bag preservation aim to shift complications management from reactive to proactive. They are designed to mechanically preserve the capsular environment and sustain the surgical options it affords over time.2
CLINICAL CASES
No. 1: Anterior Segment Stability Over 6 Months
Two patients undergoing bilateral cataract surgery received a standard monofocal IOL (AcrySof IQ [model SN60WF], Alcon) in one eye and the same IOL combined with an FOF in the fellow eye. Immediately postoperatively, anterior segment findings (IOL centration, anterior chamber depth, and capsular clarity) were indistinguishable between the two eyes.
During the following 6 months, the eyes with an FOF demonstrated expected postoperative changes. In case No. 1, progressive ACCS was observed (Figure 1). In case No. 2, IOL decentration and posterior capsular opacification were evident (Figure 2).
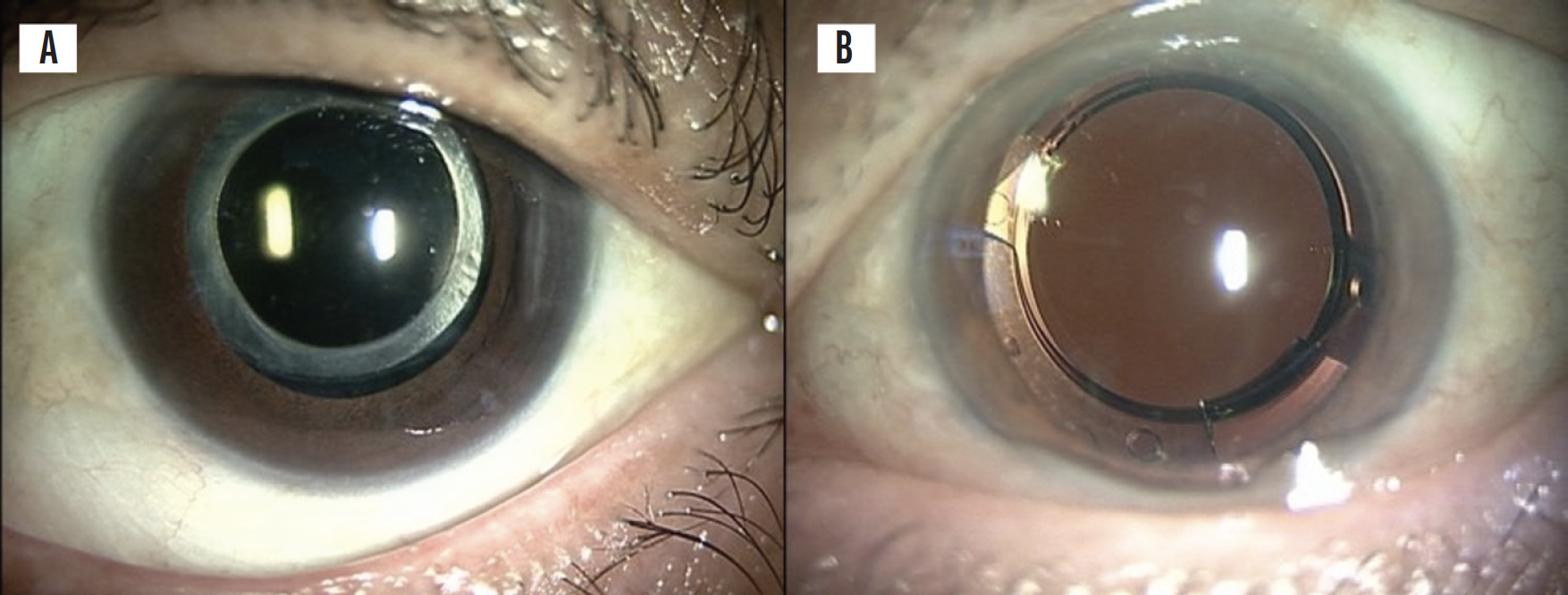
Figure 1. Anterior segment photographs obtained 6 months postoperatively in case No. 1. Standard in-the-bag implantation of an SN60WF IOL (A). SN60WF IOL implanted with an FOF (B).
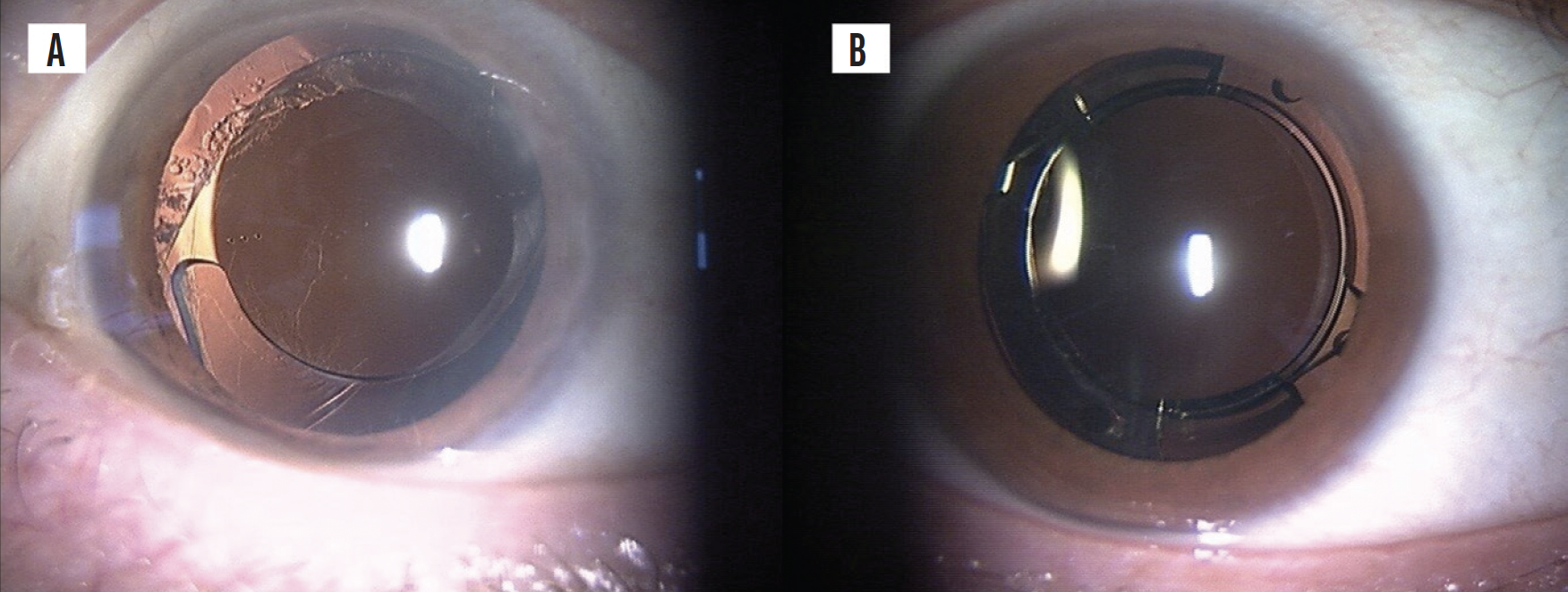
Figure 2. Anterior segment photographs obtained 6 months postoperatively in case No. 2. Standard in-the-bag implantation of an SN60WF IOL (A). SN60WF IOL implanted with an FOF (B).
The postoperative course of the eyes with an FOF was different. Capsular opacification was minimal, ACCS was avoided, and IOL centration remained essentially as it was immediately postoperatively (Figures 1 and 2). Compared with the conventional eyes, the FOF eyes demonstrated greater capsular clarity and IOL positional stability at 6 months. In my experience, conventionally implanted eyes rarely maintain this degree of capsular clarity and positional stability in this time frame.2
No. 2: IOL Exchange for Late Macular Degeneration
A patient who had received a trifocal IOL (Clareon PanOptix, Alcon) combined with an FOF presented 18 months postoperatively with a visual decline attributable to progressive age-related macular degeneration. A fundus examination and multimodal imaging confirmed macular involvement, and the treating retina specialist initiated intravitreal anti-VEGF therapy.
Given the patient’s deteriorating macular function, retention of the presbyopia-correcting IOL would have been suboptimal. An IOL exchange for a monofocal IOL was therefore performed.
Postoperatively, the patient’s corrected distance visual acuity improved modestly, and they reported clearer, more comfortable vision. This case demonstrates that, when macular pathology renders a premium IOL undesirable, the presence of an FOF can convert an otherwise clinically prohibitive situation into a manageable one (Figure 3).2

Figure 3. IOL exchange performed 18 months postoperatively. Explantation of the original IOL (A). Insertion of the replacement IOL (B). Anterior segment OCT at the time of the original IOL implantation (C). Anterior segment OCT following the implantation of the replacement IOL (D).
CLINICAL IMPLICATIONS
The cases presented herein suggest that the FOF may help reduce the occurrence of ACCS and IOL decentration and facilitate late IOL exchange. Prospective controlled data from larger patient series are required to fully characterize the long-term biocompatibility of the FOF, its influence on refractive outcomes, and the safety profile of IOL exchange procedures performed through the device.
CONCLUSION
Residual refractive error, patient dissatisfaction with premium IOLs, ACCS-induced decentration, and late macular disease represent four clinical scenarios in which the lack of a revisable IOL platform has forced surgeons and patients to accept suboptimal outcomes. Devices that preserve IOL exchangeability could expand surgeons’ ability to manage these complications whenever and however they arise.2
1. EYE PCR receives CE mark for fixOflex endocapsular device. EyePCR. Published February 12, 2026. Accessed April 7, 2026. https://www.eyepcr.com/news/eye-pcr-receives-ce-mark-for-fixoflex-endocapsular-device
2. Noguchi S, Pallikaris I. Breakthrough with artificial capsular bag in cataract surgery. Film presented at: 2024 ASCRS Annual Meeting; April 5-8, 2024; Boston, MA.