KEY TAKEAWAYS
- Middle segment surgery uses a pars plana approach to fix anterior segment problems like dislocated or subluxated IOLs—and surgeons now disagree over who should perform it.
- Proponents say success depends as much on IOL selection, scleral fixation, and refractive planning as on vitreous clearance, requiring hybrid expertise.
- Many vitreoretinal surgeons counter that formal fellowship training—widefield visualization, peripheral retinal exam, complication management—can’t be shortcut and remains essential for patient safety.
Point: Middle Segment Surgery Requires Cross-Domain Expertise
These cases should be performed by surgeons who understand vitreous management, IOL strategy, fixation biomechanics, and refractive planning.
By Sadeer B. Hannush, MD, and Kamran M. Riaz, MD


Anterior segment surgeons are familiar with the challenge of managing displaced or subluxated IOLs. These clinical entities have become increasingly common—almost to epidemic proportions—years after cataract surgery, particularly in eyes with pseudoexfoliation (PXF) syndrome (Figure) or a history of vitrectomy.1-3 History has shown that, when IOLs dislocate, especially into the vitreous cavity, they are best managed through a pars plana approach.4 Studies have shown that pars plana vitrectomy (PPV) effectively removes vitreous and lens fragments while protecting the cornea.5

Figure. Subluxated IOL–capsular bag complex with Soemmering ring in a patient with PXF syndrome.
Because many anterior segment surgeons are unfamiliar with PPV, they often refer cases of dislocated or subluxated IOLs to a vitreoretinal (VR) surgeon. This approach has inherent limitations because the VR surgeon may be less familiar with biometry, IOL properties, techniques such as sutured and sutureless scleral haptic fixation, corneal endothelial status, and the anterior segment angle, iris, and ciliary body.2
The term middle segment surgery (MSS) refers to surgery performed through the pars plana to address anterior segment pathology and surgical complications.6 Although PPV was historically the domain of the VR surgeon, MSS has evolved into a valuable technique for cornea and anterior segment specialists as well.5 Its increasing relevance across diverse clinical scenarios underscores the need for structured training and broader adoption across ophthalmic specialties.
WHY MSS EXISTS
MSS should not be limited by subspecialty boundaries. Any surgeon—anterior or posterior segment—who acquires the requisite vitrectomy and anterior segment surgical skills should be able to perform these procedures safely, and outcomes should define success.
In many contemporary MSS cases, particularly those involving scleral-fixated IOLs, visual outcomes are driven as much by IOL selection, fixation mechanics, and refractive planning as by vitreous clearance. Although inadequate vitreous management can certainly lead to serious complications, technically flawless vitrectomy alone does not guarantee good visual function if IOL-related factors are not fully considered (click here to watch Dr. Hannush retrieve a dislocated IOL–capsular bag complex from the vitreous and perform scleral fixation of a new IOL in a patient with PXF syndrome).
An important advantage of working through the pars plana is operating in a closed system. This approach allows the surgeon to control fluid mechanics. An infusion line placed through a sclerotomy maintains controlled IOP. An inadequately pressurized eye can lead to intra- and postoperative complications. There is a clear benefit in controlling fluid movement into and out of the eye during surgery.
Most anterior segment surgeons performing MSS, myself (S.B.H.) included, use VR surgical platforms such as the Constellation Vision System (Alcon), the Unity Vitreoretinal Cataract System (Alcon), and the Stellaris PC (Bausch + Lomb).
THE REQUIRED SKILL SET
Unlike procedures confined to a single domain (anterior or posterior segment surgery), MSS requires a hybrid skill set. Anterior segment surgeons must acquire proficiency in basic PPV techniques, and VR specialists must become conversant with refractive principles, IOL design, and anterior segment wound construction. All middle segment surgeons must thoroughly understand the relationships among the IOL, iris pigment epithelium, ciliary body, trabecular meshwork, and corneal endothelium.5
A core limitation for anterior segment surgeons is that they frequently lack formal training in pars plana trocar placement, the use of posterior infusion lines, and high-speed, small-gauge vitrectomy techniques. There are also specific VR instruments and devices—endoilluminators, posterior viewing systems, and endolasers—that anterior segment surgeons are not typically trained to use but can learn with proper observation and training.
Modern MSS demands a detailed understanding of IOL design, haptic architecture, and fixation biomechanics, none of which is addressed by formal VR training alone.
WHERE ANTERIOR EXPERTISE MATTERS
Historically, anterior segment surgeons had deeper expertise in IOL selection, positioning, and fixation techniques. Until about a decade ago, VR surgeons tended to place lens implants in the anterior chamber when removing posteriorly migrated lens fragments or IOLs from the vitreous cavity.4 This approach carried the risk of corneal decompensation, uveitis-glaucoma-hyphema syndrome, chronic cystoid macular edema, and glaucoma. Cornea specialists have long cautioned against this practice. VR surgeons have since made significant strides in adopting scleral-fixated posterior chamber IOL techniques such as the glued IOL technique, sutured scleral fixation, and sutureless intrascleral haptic fixation.5,7,8
That said, many contemporary MSS cases require more than vitreous clearance and lens rescue. In these eyes, the surgeon must understand the interplay among fixation strategy, IOL design, corneal status, iris integrity, angle anatomy, and endothelial health (click here to watch Dr. Hannush manage concurrent IOL dislocation and corneal endothelial disease in a single operative setting). These factors can influence not only operative safety but also long-term visual function.
For many of these patients, the surgical plan must address concurrent anterior segment pathology such as iris defects, glaucoma, and corneal disease, all of which influence both surgical technique and visual outcomes. Equally important is preventing future anterior segment complications. Careful attention to IOL design, fixation strategy (sutured vs sutureless), and the biomechanics of lens positioning can reduce long-term risks such as IOL tilt, pigment dispersion, uveitis-glaucoma-hyphema syndrome, and progressive endothelial compromise.
REFRACTIVE PLANNING
IOL power calculation and refractive targeting must be prioritized, particularly in eyes that have a history of refractive surgery, corneal ectasia, or irregular astigmatism and those for which corneal transplantation is anticipated. Reliance on legacy formulas such as the Haigis, Holladay 1, Hoffer Q, and SRK/T is inappropriate for these complex eyes, which benefit from modern formulas such as the Barrett, Cooke K6, EVO, and Kane; consideration of posterior corneal power (eg, total keratometry); post–refractive surgery formulas; and careful consideration of shifts in effective lens position inherent to scleral fixation techniques.
Refractive Targeting
Refractive targets often must be adjusted when concurrent or future corneal surgery is likely. Endothelial and penetrating keratoplasty are known to induce systematic refractive shifts, and the failure to account for this can leave patients with significant refractive errors despite successful VR outcomes. These decisions are central determinants of patient satisfaction and long-term visual function.
Advanced Options
Advanced MSS increasingly includes the scleral fixation of toric IOLs to address preexisting corneal astigmatism and, in select cases, the implantation of a Light Adjustable Lens (RxSight) to allow postoperative refractive titration. These approaches prioritize refractive optimization and require expertise in preoperative planning and postoperative visual rehabilitation—traditional domains of anterior segment training.
COLLABORATION AND CASE SELECTION
Collaboration remains valuable, but the surgeon performing MSS must understand more than vitreous access alone. Anterior segment surgeons can expand their capabilities by observing VR colleagues in surgery and developing a facility with posterior segment instrumentation and techniques. VR surgeons who perform these cases should understand the biometric, refractive, and anterior segment considerations that influence lens choice and fixation as well as long-term visual function.
Posterior segment instrumentation should be available whenever these cases are undertaken, and the operating surgeon must be prepared to identify retinal pathology, manage complications, and obtain prompt VR assistance when needed. Conversely, inadequate access to contemporary biometry and refractive planning tools can compromise outcomes even when the VR portion of the surgery is technically successful.
Finally, the anterior segment surgeon should have ready access to a VR surgeon in the event that their assistance is required either to complete the case or to examine the patient the following day. Surgeons performing MSS must develop a familiarity with both anterior and posterior segment principles—ideally through dedicated training and observation—or approach these cases collaboratively, with VR and anterior segment surgeons working together to optimize outcomes for patients with complex anterior segment problems.
CONCLUSION
MSS is often described as removing vitreous and implanting a new IOL, but it is far more nuanced. Most cases do not require total vitrectomies. Adequate IOP control and avoidance of hypotony are critical to success. Moreover, evidence suggests that preserving residual vitreous may benefit long-term IOL stability, IOP control, and visual outcomes.9-12 Success depends on the safe removal of sufficient vitreous, stable IOL fixation, and sophisticated refractive planning. The development of IOL power calculation formulas that better model effective lens position, the incorporation of posterior corneal curvature, and thoughtful refractive targeting have transformed what were once salvage operations.
For these reasons, successful MSS requires a broad skill set that can be learned by both anterior and posterior segment surgeons interested in complex IOL cases.
1. Kristianslund O, Dalby M, Drolsum L. Late in-the-bag intraocular lens dislocation. J Cataract Refract Surg. 2021;47(7):942-954.
2. Hannush SB. Sutured posterior chamber intraocular lenses: indications and procedure. Curr Opin Ophthalmol. 2000;11(4):233-240.
3. Ifantides C, Hannush SB, Fram NR, et al. Middle segment surgery: a new frontier for anterior segment surgeons. Presented at: ASCRS ASOA Annual Meeting; April 5-8, 2024; Boston, MA.
4. Starr MR, Weng CY, Vajzovic L, Blinder KJ, Kim JE, Jumper JM. Approach to ophthalmic surgery involving the anterior vitreous: a clinical practice update from the American Society of Retina Specialists. J Vitreoretin Dis. 2025;9(6):744-750.
5. Hannush SB. Corneal considerations for noncapsular IOL fixation. In: Chang DF, ed. Advanced IOL Fixation Techniques: Strategies for Compromised or Missing Capsular Support. CRC Press; 2024:463-468.
6. Hannush SB, Chayet A, Ifantides C. Middle segment surgery: indications, techniques, and future directions. Curr Opin Ophthalmol. 2026;37(1):25-30.
7. Kumar DA, Agarwal A. Glued intraocular lens: a major review on surgical technique and results. Curr Opin Ophthalmol. 2013;24(1):21-29.
8. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136-1142.
9. Gallo Afflitto G, Fabozzi L, Palmieri F, et al. Ocular hypertension and glaucoma after pars plana vitrectomy: a systematic review and meta-analysis. Ophthalmology. 2026;133(3):387-398.
10. Zong Y, Gao QY, Hui YN. Vitreous function and intervention of it with vitrectomy and other modalities. Int J Ophthalmol. 2022;15(6):857-867.
11. Kaufmann GT, Gupta O, Yu J, et al. Vitreoretinal Outcomes Following Secondary Intraocular Lens Implantation with Pars Plana Vitrectomy. Retina. 2024;44(8):1337-1343.
12. Yamada M, Nishimura E, Watanabe S, et al. Comparison of complications of intrascleral fixation according to the extent of vitrectomy. BMC Ophthalmol. 2024;24(1):1-5.
Counterpoint: Complex Pars Plana Cases Require Vitreoretinal Training
Surgery is safest in the hands of ophthalmologists with formal vitreoretinal training and expertise in visualization, peripheral retinal examination, and complications management.
By Matthew R. Starr, MD

A recent trend in ophthalmic surgery among surgeons without vitreoretinal (VR) fellowship training involves the middle segment of the eye, defined as the area 2 to 4 mm posterior to the surgical limbus and surrounding the vitreous base insertion.1 Proponents argue that the anatomy is secondary to the concept: a single surgeon performs both the anterior and posterior approaches in complex pars plana cases.1 They further contend that a pars plana approach using anterior or subtotal vitrectomy is the best technique in some of these cases and that a total vitrectomy is not always necessary.1 In response, the American Society of Retina Specialists published a white paper detailing the retina community’s concerns about the use of VR surgical techniques by surgeons without VR training.2
The retina community’s concerns center on four principles:
- No. 1: VR surgical training;
- No. 2: Widefield vitreous cavity visualization;
- No 3: Appropriate examination of the ora serrata; and
- No. 4: Patient safety.
COMPETING CLAIMS
Patient safety and outcomes drive the debate. Anterior segment surgeons argue that VR surgeons who perform secondary IOL surgery in this space should strengthen their understanding of biometry, anterior segment OCT, limbal wound creation, how to avoid glaucoma and endothelial cell damage, IOL properties, and scleral fixation techniques.3 They also argue that surgeons without VR fellowship training must understand trocar placement, posterior segment visualization, small-gauge vitrectomy platforms, scleral wound closure, peripheral retinal visualization, the management of anticoagulated patients and associated hemorrhage or hypotony, and the use of perfluorocarbon liquid (PFCL) to levitate lenses or retained lens fragments.3
TRAINING AND EXPERIENCE
Surgical retina is a well-established ophthalmic subspecialty that requires 2 years of postresidency training, with standards developed by the Association of University Professors in Ophthalmology Fellowship Compliance Committee in coordination with the American Society of Retina Specialists, the Macula Society, and the Retina Society.4
Surgical retina fellows often graduate with nearly 1,000 surgical cases, yet the learning curve for VR surgery extends years into practice.5,6 It is unrealistic to condense even a small portion of VR surgical techniques—and certainly the recognition and management of their complications—into a weekend training course, as proponents of this middle segment approach have suggested.7
What VR Training Already Covers
With recent IOL technologies and better integration of biometry into ophthalmology residency training, VR surgeons are routinely exposed to biometry, lens calculations, refractive principles, and anterior segment surgery during a 4-year ophthalmology training program.8 They then acquire VR surgical principles during a 2-year VR fellowship, during which mentors guide them on the management of both the anterior and the posterior segment because of the complexity of the diseases encountered during VR training.8
What Residency Does Not Provide
Ophthalmology residency does not include surgical requirements for performing VR surgery. Trainees are expected to assist in at least 10 VR surgical cases, which is why a 2-year surgical fellowship is necessary to acquire the skills required to perform VR surgery independently.4
SURGICAL REQUIREMENTS
Visualization and Peripheral Examination
For these cases, widefield illumination, complete pars plana vitrectomy (PPV), and a peripheral retinal examination using scleral depression are paramount. VR surgeons use sophisticated wide-angle viewing systems to visualize the anterior vitreous and peripheral retina. These include contact lenses,9 noncontact lens viewing systems,10 and 3D heads-up display systems.11 Although these systems provide excellent views of the peripheral retina, simultaneous scleral depression is often required to visualize the entire periphery so that tears, holes, and other retinal defects can be identified and treated.
Preoperative retinal breaks identified with scleral depression and intraoperative retinal breaks occur in approximately 5% to 8% of routine VR surgical cases and in up to 20% of cases involving vitreomacular traction or macular holes.12-14 Because standard operating microscopes alone do not permit a complete retinal evaluation, especially during single-port vitrectomy, pathology may be missed. A peripheral retinal examination using scleral depression is a routine step in conventional PPV performed by VR surgeons.
PFCL Use
The notion of using PFCL to elevate material within the vitreous cavity is untenable. PFCL use requires a complete PPV with the induction of a posterior vitreous detachment, followed by complete removal under posterior segment visualization. Long-term retention of PFCL in the eye can lead to chronic inflammation, secondary glaucoma, retinal pigment epithelium toxicity, retinal thinning, and corneal endothelial decompensation.15-18 PFCL in the vitreous cavity can therefore have unintended consequences if it is not completely removed.
LIMITS OF SUBTOTAL VITRECTOMY
Appropriate Uses
Many non-VR surgeons perform an anterior vitrectomy through a pars plana approach with modern vitrectomy platforms and achieve safe outcomes.19 Non-VR surgeons also use pars plana approaches in situations beyond secondary IOL surgery, including aqueous misdirection, anterior chamber flattening, and cases that require posterior infusion or vitreous decompression.3 These maneuvers can be safer for patients when performed through a pars plana approach. A limited anterior vitrectomy, however, may lead to adverse outcomes when a complete PPV is required and appropriate techniques are not used.20
Cases Requiring Complete Vitrectomy
Some non-VR surgeons may choose subtotal vitrectomy for vitreous hemorrhage, vitreous biopsy, pars plana tube shunts, vitreous prolapse into the anterior chamber, or symptomatic vitreous opacities—all conditions that require a complete vitrectomy. The last of these has already been reported in an office setting with a single-port vitrectomy machine.21 Even when vitreous floaters are removed with a PPV, the return-to-the-OR rate has been reported to exceed 3%, and rhegmatogenous retinal detachment has been reported in up to 11% of eyes.22-25
WHO SHOULD HANDLE COMPLEX CASES?
Refractive and Anatomic Outcomes
In many cases, the goal of VR surgery is anatomic restoration.26-28 Non-VR surgeons cite this as an area in which VR surgeons must improve when refractive and visual outcomes take priority.3 Retina surgeons, however, have moved away from anterior chamber IOLs when performing secondary IOL surgery and achieve refractive outcomes similar to those of anterior segment surgeons.29-31 As retina surgeons perform more of these surgeries and achieve strong refractive and anatomic outcomes, the need for combined cases may become limited.
Referral Thresholds
Many retina surgeons, like many anterior segment surgeons, do not wish to perform these procedures. The procedures should therefore be performed by surgeons who perform them regularly and can manage intra- and postoperative complications. In general, anterior segment surgeons can manage complex lens cases when the lens has not completely dislocated into the vitreous cavity. Dr. Hannush has acknowledged the need for VR support: “The anterior segment surgeon should cooperate with and have access to a [VR] surgeon in the event there is a problem requiring the assistance of the VR surgeon either to complete the case or to send the patient to the [VR] specialist the following day.”3 Debate over.
CONCLUSION
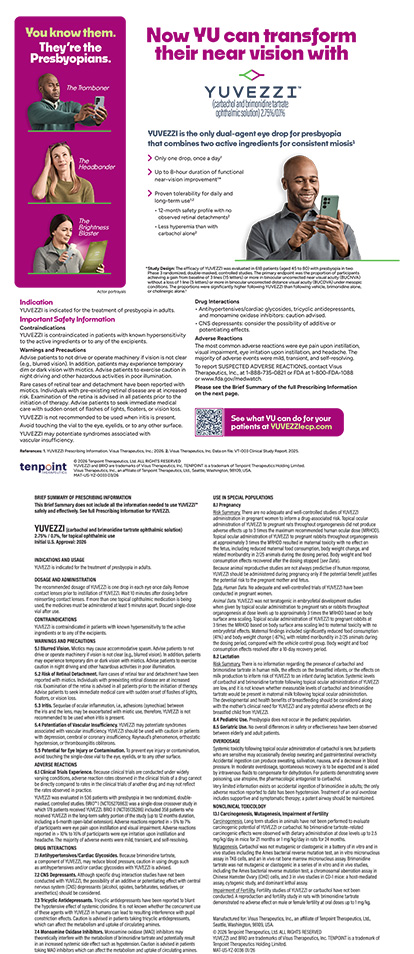
Non-VR and VR surgeons share the goal of achieving the best possible outcome with the fewest procedures for patients who have extensive anterior and posterior segment pathology. When a PPV is required, the best approach may be combined surgery or separate procedures. Many of these cases, however, can be performed safely by VR surgeons alone, with strong anatomic and refractive outcomes (Figure).
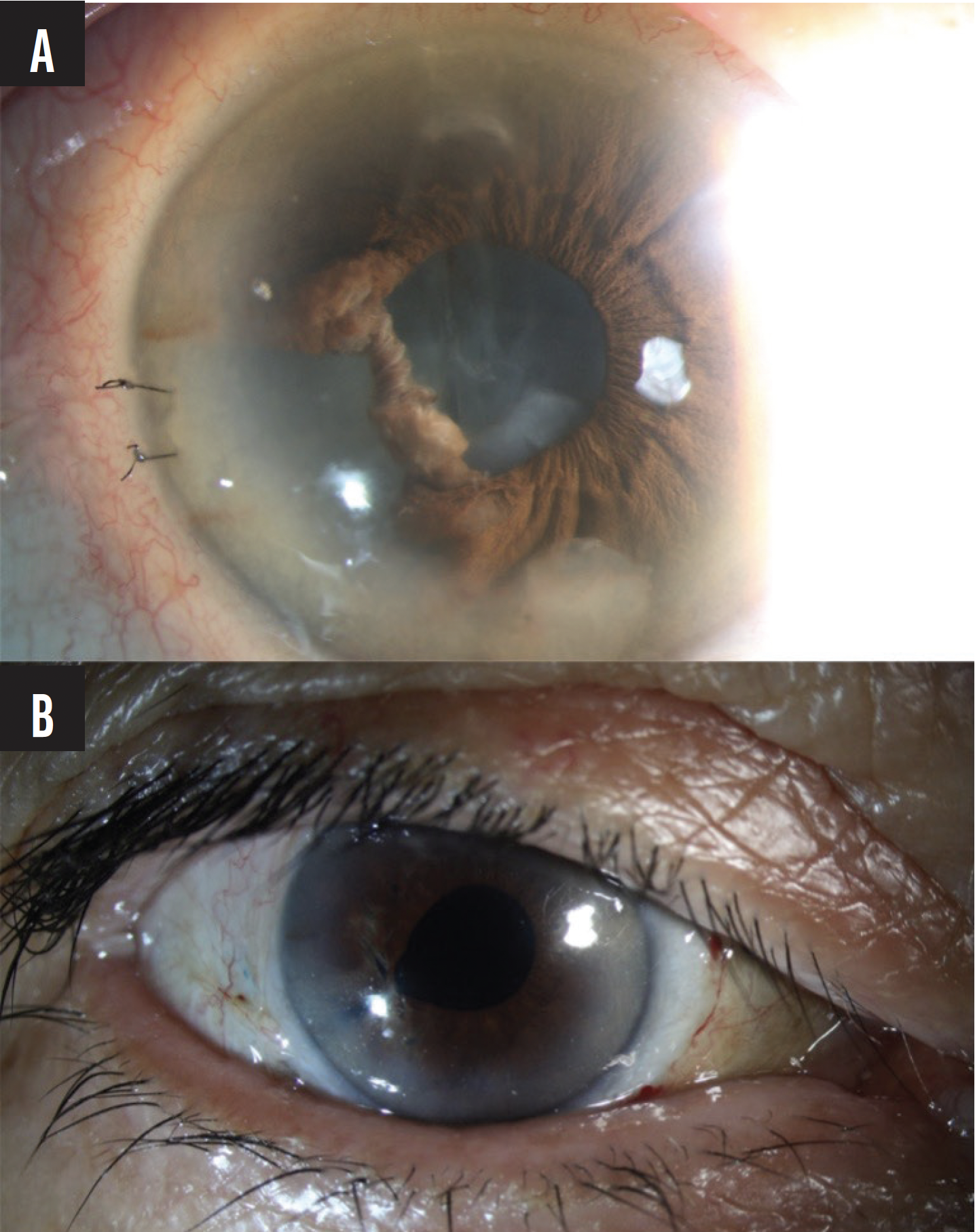
Figure. Complex cataract surgery with retained lens material, aphakia, and iris damage (A), followed by pars plana lensectomy and vitrectomy, secondary lens implantation, and iris repair by a single VR surgeon; the patient achieved a visual acuity of 20/20 (B).
1. Hannush SB, Ifantides C, Trinh T, Oliver S. Is it time for middle segment surgery? Review of Ophthalmology. May 4, 2023. Accessed April 7, 2026. https://www.reviewofophthalmology.com/article/is-it-time-for-middle-segment-surgery
2. Starr MR, Weng CY, Vajzovic L, Blinder KJ, Kim JE, Jumper JM. Approach to ophthalmic surgery involving the anterior vitreous: a clinical practice update from the American Society of Retina Specialists. J Vitreoretin Dis. 2025;9(6):744-750.
3. Hannush SB, Chayet A, Ifantides C. Middle segment surgery: indications, techniques, and future directions. Curr Opin Ophthalmol. 2026;37(1):25-30.
4. Association of University Professors of Ophthalmology Fellowship Compliance Committee. Surgical retina and vitreous. AUPOFCC. Accessed June 20, 2024. https://aupofcc.org/fellowship-programs-residentssubspecialties/surgical-retina-and-vitreous
5. Bakri SJ, Alniemi ST, Chan RV. Experiences of vitreoretinal surgery fellows in the United States. Retina. 2013;33(2):392-396.
6. Williams GA. Vitreoretinal surgery fellowship training and the big disconnect: Is it just a numbers game? Retina. 2013;33(2):263-264.
7. Belin PJ, Parke DW 3rd. Complications of vitreoretinal surgery. Curr Opin Ophthalmol. 2020;31(3):167-173.
8. Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Ophthalmology. Revised September 2025; effective July 1, 2026. Accessed April 7, 2026. https://www.acgme.org/globalassets/pfassets/programrequirements/2026-prs/240_ophthalmology_2026.pdf
9. Peyman GA. A new wide-angle irrigating contact lens for pars plana vitrectomy. Can J Ophthalmol. 1988;23(3):150.
10. Landers MB, Peyman GA, Wessels IF, Whalen P, Morales V. A new, non-contact wide field viewing system for vitreous surgery. Am J Ophthalmol. 2003;136(1):199-201.
11. Eckardt C, Paulo EB. Heads-up surgery for vitreoretinal procedures: an experimental and clinical study. Retina. 2016;36(1):137-147.
12. Jairath NK, Paulus YM, Yim A, et al. Intra- and post-operative risk of retinal breaks during vitrectomy for macular hole and vitreomacular traction. PLoS One. 2022;17(8):e0272333.
13. Subedi S, Sharma MK, Sharma BR, Kansakar I, Dhakwa K, Adhikari RK. Surgical outcome of pars plana vitrectomy: a retrospective study in a peripheral tertiary eye care centre of Nepal. Nepal J Ophthalmol. 2010;2(1):39-44.
14. Moore JK, Scott IU, Flynn HW Jr, et al. Retinal detachment in eyes undergoing pars plana vitrectomy for removal of retained lens fragments. Ophthalmology. 2003;110(4):709-713; discussion 713-714.
15. Lesnoni G, Rossi T, Gelso A. Subfoveal liquid perfluorocarbon. Retina. 2004;24(1):172-176.
16. Shulman M, Sepah YJ, Chang S, Abrams GW, Do DV, Nguyen QD. Management of retained subretinal perfluorocarbon liquid. Ophthalmic Surg Lasers Imaging Retina. 2013;44(6):577-583.
17. Tewari A, Eliott D, Singh CN, Garcia-Valenzuela E, Ito Y, Abrams GW. Changes in retinal sensitivity from retained subretinal perfluorocarbon liquid. Retina. 2009;29(2):248-250.
18. Yu Q, Liu K, Su L, Xia X, Xu X. Perfluorocarbon liquid: its application in vitreoretinal surgery and related ocular inflammation. Biomed Res Int. 2014;2014:250323.
19. Thornton IL, McMains BK, Snyder ME. Long-term safety and efficacy of single-port pars plana anterior vitrectomy with limbal infusion during anterior segment surgery. J Cataract Refract Surg. 2018;44(7):878-883.
20. Naderi K, Allen F, Dowlut S, Karia N, Chandra A. The risk of rhegmatogenous retinal detachment following anterior vitrectomy during cataract surgery: with versus without pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol. 2020;258(11):2425-2429.
21. Banas J, Schiffbauer J. Step into the vitreous. Review of Optometry. 2023;160(12). Accessed April 7, 2026. https://www.reviewofoptometry.com/article/step-into-the-vitreous
22. Henry CR, Schwartz SG, Flynn HW Jr. Endophthalmitis following pars plana vitrectomy for vitreous floaters. Clin Ophthalmol. 2014;8:1649-1653.
23. Radke N, Lam DSC. Floaterectomy—risks, safety, and future. Asia Pac J Ophthalmol (Phila). 2017;6(3):304.
24. Rubino SM, Parke DW 3rd, Lum F. Return to the operating room after vitrectomy for vitreous opacities: Intelligent Research in Sight Registry analysis. Ophthalmol Retina. 2021;5(1):4-8.
25. Ryan EH. Current treatment strategies for symptomatic vitreous opacities. Curr Opin Ophthalmol. 2021;32(3):198-202.
26. Heegaard S. Morphology of the vitreoretinal border region. Acta Ophthalmol Scand Suppl. 1997;(222):1-31.
27. Sebag J. Anatomy and pathology of the vitreo-retinal interface. Eye (Lond). 1992;6(pt 6):541-552.
28. Trese M, Chandler DB, Machemer R. Macular pucker. II. Ultrastructure. Graefes Arch Clin Exp Ophthalmol. 1983;221(1):16-26.
29. Bantounou MA, Aggarwal N, Boucher N, Sharma C, Starr MR. Trends and outcomes of secondary intraocular lens utilization among vitreoretinal surgeons compared to vitreoretinal and anterior segment surgeons. Ophthalmic Surg Lasers Imaging Retina. 2025;56(10):602-607.
30. Kaufmann GT, Boucher N, Sharma C, Starr MR. Trends in secondary intraocular lens surgery among vitreoretinal surgeons. Ophthalmol Retina. 2023;7(11):965-971.
31. Kaufmann GT, Gupta O, Yu J, et al. Vitreoretinal outcomes following secondary intraocular lens implantation with pars plana vitrectomy. Retina. 2024;44(8):1337-1343.