


CASE PRESENTATION
A 25-year-old woman is referred for a decrease in the quality and quantity of vision in her right eye. The patient’s history is significant for bilateral LASIK performed 4 years ago, followed by a PRK enhancement in the right eye only.
Her BCVA is 20/25 OD with a manifest refraction of -0.25 D sphere and 20/20 OS with a plano manifest refraction. Her UCVA is 20/25 OD and 20/20 OS.
Pachymetry is 409 µm OD. Grade 2 to 3 corneal haze is evident in the right eye (Figure 1). An analysis with the Pentacam (Oculus Optikgeräte) shows normal surface topography (Figure 2) but also reduced contrast sensitivity and haze in the right eye (Figure 3).

Figure 1. A slit-lamp examination reveals corneal haze 9 months following a PRK enhancement.

Figure 2. Pentacam analysis of the topographic changes and haze.

Figure 3. Scheimpflug tomography shows the extent and depth of the haze.
The rest of the ocular examination is unremarkable except for bilateral dry eye disease (DED). Staining with lissamine green is moderate, and the tear breakup time is 4 seconds in each eye. Additionally, both eyes have meibomian gland dysfunction (MGD) grade +3 or +4, and a limited amount of meibum can be expressed from the eyelids.
The patient has received multiple courses of therapy with isotretinoin (Accutane, Roche) for the treatment of severe acne vulgaris.
Aggressive DED therapy improves the ocular surface and optical quality in both eyes (Figures 4 and 5). Nevertheless, the UCVA of the patient’s dominant right eye is still decreased. She requests further intervention. What, if anything, would you do to improve the quality and quantity of vision and contrast sensitivity in the right eye?
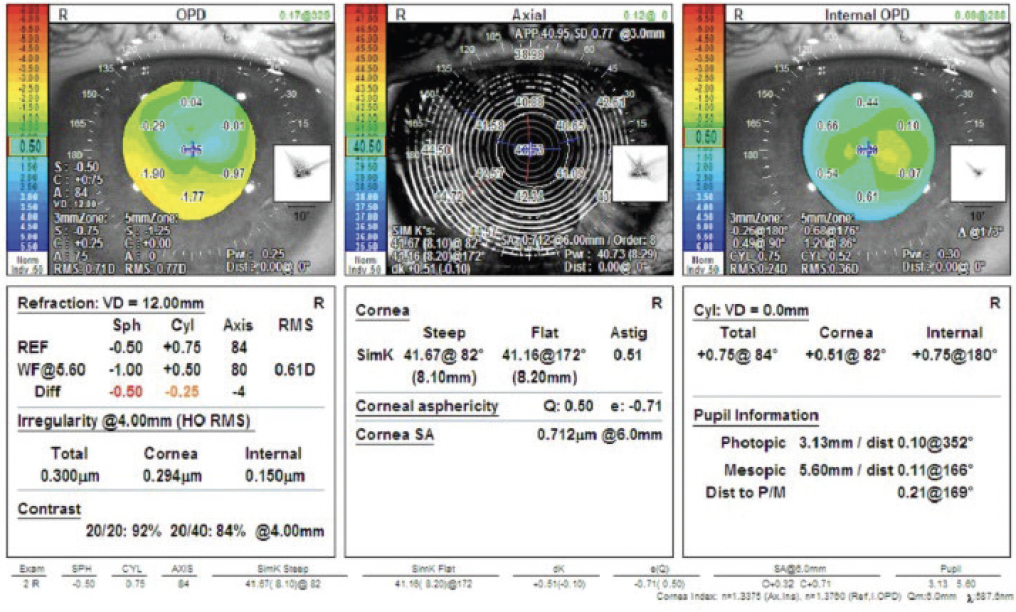
Figure 4. Measurements of the tear film quality, higher-order aberrations, contrast sensitivity, and corneal irregularity index with the OPD-Scan III (Nidek).

Figure 5. An analysis with the Damian Gatinel Optical Quality Analysis Software on the OPD-Scan III shows changes related to the corneal higher-order aberrations.
—Case prepared by Karl G. Stonecipher, MD

MICHAEL D. GREENWOOD, MD
Aggressive DED treatment would be either initiated or continued. I want to ensure that the meibomian glands are functioning and would employ a combination of thermal and mechanical therapies to accomplish this goal. Topical cyclosporine therapy would be prescribed to address underlying inflammation. Treatment with a potent topical steroid such as dexamethasone would also be started in an effort to resolve the haze. If this course of steroids does not improve the corneal haze and reduce the patient’s visual complaints, a superficial keratectomy with topical mitomycin C (MMC) would be performed. Should the procedure fail to clear the haze, then a phototherapeutic keratectomy (PTK) with MMC could be performed.
The patient would be counseled that the haze may recur and that her refractive error may change depending on healing. The aforementioned strategies should, however, resolve the visual quality issues.

MARK A. KONTOS, MD
The good news is that there are treatment modalities that should improve the vision in the patient’s right eye. The bad news is that it is going to take some time to resolve the issue.
If not already attempted, a 3-month trial of steroid treatment would be conducted to reduce the haze. If no improvement occurs, a PTK with a prolonged application of MMC (0.02% for 2 minutes) would be performed. Epithelial mapping would assist with planning the treatment depth. The goal would be to remove as much haze as possible while preserving as much corneal tissue as possible. CXL could also be considered if a refractive PRK procedure is planned for the future.
It would be important to explain to the patient that her uncorrected distance visual acuity is likely to worsen (become more hyperopic) in the short term after PTK treatment. I would counsel her to protect the eye from UV light and would consider prescribing a vitamin C supplement. If there is resolution of the haze, further refractive PRK could be considered 6 months after the PTK procedure.

WILLIAM B. TRATTLER, MD
Late-onset corneal haze in the right eye has reduced the patient’s quality of vision and caused some irregular astigmatism that is evident on Pentacam analysis. Her main risk factors for developing haze included undergoing PRK over a previous LASIK flap and significant ocular surface disease/MGD. UV light exposure is another risk factor for haze formation,1 although her level of exposure is not described.
Late-onset corneal haze is distinct from haze related to delayed epithelial healing following PRK. Parag Majmudar, MD, has shown that adjunctive MMC can effectively reduce the risk of haze formation and can be administered intraoperatively to eyes that are at increased risk of late-onset corneal haze, such as those with a history of corneal surgery (eg, LASIK, PRK, intrastromal corneal ring segments) and those that received a deep ablation.2,3 These eyes exhibit a reticular pattern of corneal haze (Figure 1) that typically reduces the patient’s BCVA and causes a myopic shift. In my experience, individuals with MGD and/or blepharitis are at increased risk of developing late-onset corneal haze.
MGD treatment would be continued. Medical therapy to address the corneal haze has a good chance of success because the patient has experienced only a mild loss of BCVA. Therapy with prednisolone acetate 1% four times per day and hypochlorous acid spray to the eyelashes twice daily would be initiated. I would also prescribe topical losartan six times per day based on the findings of Dr. Wilson.4 Additionally, I would strongly encourage the patient to undergo treatment with the Lipiflow Thermal Pulsation System (Johnson & Johnson Vision), TearCare System (Sight Sciences), or iLux (Alcon) or intense pulsed light therapy to address the significant MGD.
She would be asked to return every 3 to 4 weeks for 3 to 4 months to monitor her response to treatment. If the haze and signs and symptoms of ocular surface disease improve, I would expect her to experience a reduction in myopia, an increase in quality of vision, and a decrease in reticular haze that is visible at the slit lamp and with corneal OCT imaging.

STEVEN E. WILSON, MD
My approach would depend on the timing of the PRK enhancement in the right eye. The slit-lamp photograph (Figure 1) shows that lacunae have developed in the fibrotic haze. (The clear areas within the haze are where the epithelial basement membrane [EBM] has been fully regenerated via the coordinated efforts of corneal epithelial cells and corneal fibroblasts.) Myofibroblasts have undergone apoptosis, and corneal fibroblasts/keratocytes have migrated into the fibrotic tissue to reabsorb/reorganize the disordered collagens and other matrix materials secreted by the myofibroblasts.5 Normally, these lacunae continue to enlarge and coalesce until full stromal transparency returns. Thus, if the patient’s visit is relatively soon (< 6 months) after the PRK retreatment, I would observe her for the next 6 months to see if there is further spontaneous clearing. Conversely, if the PRK retreatment was performed closer to the time of the original LASIK surgery 4 years ago or if PRK occurred more recently but there have been no signs of further clearing, then treatment with topical 0.8 mg/mL of losartan six times per day obtained from a compounding pharmacy would likely be beneficial.4
The persistence of the fibrotic haze in the cornea indicates that viable myofibroblasts continue to populate this tissue years after the original injury. Losartan inhibits transforming growth factor (TGF) beta signaling inside the cell at the signal transduction protein extracellular signal-regulated kinase (ERK) and triggers the apoptosis of residual myofibroblasts that depend on adequate and ongoing TGF-beta signaling for survival. Additionally, losartan likely blocks the development of new myofibroblasts from corneal fibroblasts or bone marrow–derived fibrocytes that are also driven by TGF-beta signaling to transition into mature myofibroblasts.
This function of cutting off TGF-beta 1 signaling to the stroma from the tears and corneal epithelium is normally performed by the EBM via its perlecan component, which repels TGF-beta owing to its molecular charge, and collagen type IV, that binds TGF-beta and prevents it from binding to TGF-beta receptors.4 The development and persistence of fibrosis in this case indicate that, for some reason, EBM regeneration was defective and myofibroblasts still occupy these hazy fibrotic areas in the stroma between the lacunae. Myofibroblasts cannot cooperate with epithelial cells to regenerate the EBM.6 Once the myofibroblasts are removed by apoptosis, however, corneal fibroblasts can move into the fibrotic tissue to facilitate final regeneration of the EBM and remove the disordered collagens and other extracellular matrix materials that contribute to the opacity.
Importantly, therapy with topical losartan (oral losartan has no effect5) must be continued for up to 6 months after the scar disappears to allow sufficient time for full EBM regeneration. Otherwise, myofibroblasts—and the disordered extracellular matrix they produce—will begin to reaccumulate. In some patients, the EBM may never regenerate despite a year or more of topical losartan treatment, and the fibrosis repeatedly recurs after therapy is discontinued. In this situation, lamellar or full-thickness corneal transplantation may become necessary. I would not recommend PTK with MMC in these eyes that have already demonstrated defective EBM regeneration after PRK because there is a high risk that worse fibrosis will recur.

WHAT I DID: KARL G. STONECIPHER, MD
After a discussion, the patient and I elected to continue aggressive DED therapy. Treatment included cyclosporine ophthalmic solution 0.1% (Vevye, Harrow) and perfluorohexyloctane ophthalmic solution (Miebo, Bausch + Lomb) in both eyes twice daily. Punctal occlusion with silicone plugs was performed bilaterally. Additionally, topical losartan 0.8 mg/mL was instilled in the affected eye six times per day for 3 months.
The patient’s UCVA improved to 20/20, and she reported a dramatic improvement in her quality of vision. The aforementioned medical therapy will be continued for another 6 months, at which time losartan treatment will be discontinued.
1. Stojanovic A, Nitter TA. Correlation between ultraviolet radiation level and the incidence of late-onset corneal haze after photorefractive keratectomy. J Cataract Refract Surg. 2001;27(3):404-410.
2. Majmudar PA, Brenart R, Epstein RJ. Topical mitomycin-C for massive subepithelial fibrosis following radial keratotomy. Cornea. 1998;17:242-243.
3. Raviv T, Majmudar PA, Dennis RF, Epstein RJ. Mitomycin-C for post-PRK corneal haze. J Cataract Refract Surg. 2000;26(8):1105-1106.
4. Wilson SE. Topical losartan: practical guidance for clinical trials in the prevention and treatment of corneal scarring fibrosis and other eye diseases and disorders. J Ocul Pharmacol Ther. 2023;39(3):191-206.
5. Marino GK, Santhiago MR, Santhanam A, Torricelli AAM, Wilson SE. Regeneration of defective epithelial basement membrane and restoration of corneal transparency. J Refract Surg. 2017;33(5):337-346.
6. Shiju TM, Sampaio LP, Hilgert GSL, Wilson SE. Corneal epithelial basement membrane assembly is mediated by epithelial cells in coordination with corneal fibroblasts during wound healing. Mol Vis. 2023;29:68-86.

