


Foreward: Welcome to CRST’s Global Perspectives column, a new initiative we’re undertaking to help eye care professionals keep up to date and informed about ophthalmic practice patterns throughout the world. There is no better time than the present to expand our scope of coverage, as we have recently been reminded by the significant increase in virtual communication and education how much we have to learn from one another and how important it is to stay connected.
Under the guidance of Jodhbir S. Mehta, BSc (Hons), MBBS, PhD, FRCOphth, FRCS(Ed), FAMS, each month Global Perspectives will review a topic of interest for anterior segment surgeons through the responses of surgeons from around the world. The goal of Global Perspectives is to cultivate the insights and practice patterns of surgeons from North America, South America, Europe, Asia, India, the Middle East, and South Africa in one place for easy dissemination.
Read this first column for a deep dive into what laser refractive surgery volume has looked like for these surgeons since the start of the COVID-19 pandemic.
Laura Straub | Editor-in-Chief
In Hong Kong, Volume is higher than pre-COVID
John S.M. Chang, MD
Hong Kong, China

During the initial outbreak of COVID-19 in January 2020, patient volume decreased by approximately 10% at the refractive surgery center in Hong Kong where I practice. Since then, despite three more community outbreaks, volume is in fact higher than in 2019 (Figure). We are busier than ever—at one point, our case volume increased by 80% compared to the previous year.
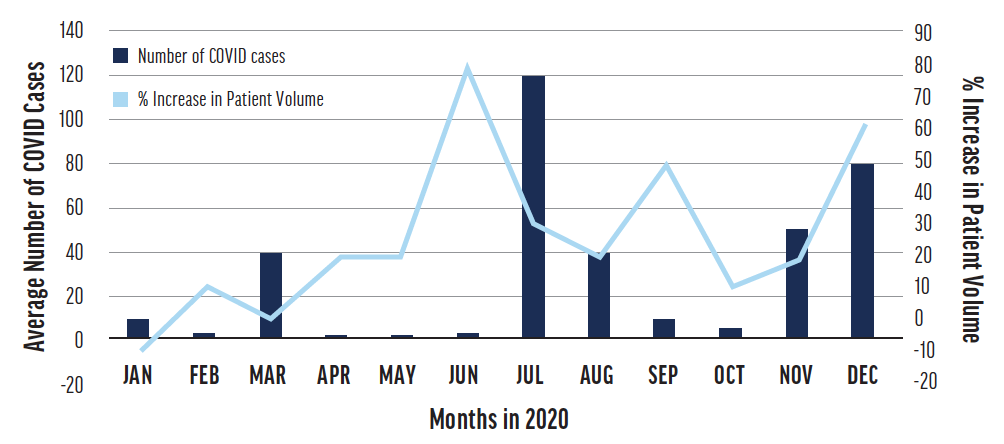
Figure. The percentage increase in refractive surgery volume in Hong Kong compared to the same months in 2019.
Source: https://www.coronavirus.gov.hk/
At our clinic, in general, patient volume is at least 10% to 20% higher compared to the same time during the previous year. In the first two outbreaks, patient volume declined immediately. During the most recent outbreak, however, patient volume increased by 60% compared with the same time the previous year; a community outbreak no longer seems to affect surgical volume.
REASONS FOR INCREASED SURGICAL VOLUME
I see five possible reasons for increased surgical volume.
No. 1: Younger patients are still presenting for refractive surgery. Compared to older patients, younger patients are less concerned about contracting SARS-CoV-2 because their mortality rate is very low.
No. 2: Young patients may not be living with elderly family members, thus reducing the risk that the former will infect the latter. There has been a noticeable drop in presbyopic LASIK patients, however, because real estate in Hong Kong is extremely expensive and these older patients are more likely to be living with elderly parents.
No. 3: Most patients are working from home right now. In many cases, this means they can undergo surgery without needing to officially take time off work.
No. 4: Spending more time at home has made many people more attentive to their general health. As a result, they are more likely to be aware of their ocular and other health problems and thus more inclined to spend money on improving their health, including through refractive surgery.
No. 5: Wearing a mask can cause glasses to fog up. Mask wear can also cause or exacerbate acne and dry eye disease.
READ IT!
Revisit thoughts on the COVID-19 pandemic shared by Dr. Chang and others in the June 2020 issue of CRST.
CHANGES IN OUR CLINIC
In our clinic, when patients book surgery or an eye examination, they answer health-related questions (more details are available in the June 2020 issue1) and undergo strict screening. Only one companion is allowed per patient. If either person has recently been somewhere with confirmed cases of COVID-19, a negative antigen test result is required. All doctors and staff members who work at the clinic or hospital receive a rapid COVID-19 antigen test weekly.
The health profiles and temperatures of patients presenting for surgery are recorded. New masks are provided for them to wear upon entering the surgery area to avoid outside contamination. These masks are worn throughout the laser procedure. Tape is firmly applied to the upper part of the mask to prevent patients’ breath from reaching their eyes. The eyelids and the taped area are disinfected with povidone-iodine before patients are brought into the OR.
The intraoperative risk of SARS-CoV-2 transmission during surface ablation, particularly transepithelial PRK, is a concern. With some excimer laser platforms, the plume evacuation system can be turned on first and allowed to run for a few seconds, creating a current that may pull the entire laser plume into the extractor.
1. Carones AC, Carones F, Chang JSM, Findl O, Mehta JS, Ang M. Global perspectives. Cataract & Refractive Surgery Today. June 2020. Accessed January 19, 2021. https://crstoday.com/articles/2020-june/global-perspectives/?single=true
A Gradual and Steady Increase Is Occurring in India
Mahipal Singh Sachdev, MD
New Delhi, India

The COVID-19 pandemic has changed the world as we know it, including practice guidelines across global ophthalmologic societies. Especially hard hit was the field of refractive surgery. Initial lockdowns required a complete cessation of nonessential ophthalmic services for more than a month, during which time no refractive surgical procedures could be planned. The equipment for refractive surgery is expensive, as is its maintenance. In addition to these unavoidable costs were those of personal protective equipment, sanitizers, and face masks.
As restrictions were partially lifted, global ophthalmologic societies scrambled to establish and balance guidelines for safe ophthalmic practice while battling the COVID-19 pandemic.
In India, the virus-related lockdown was followed by a slump in refractive surgical volume, especially during the second quarter of 2020. Some of the downturn was due to travel restrictions on patients and their apprehension at visiting health care facilities. Other factors included a huge hit to medical tourism and widespread unemployment and salary cuts, which deterred many prospective patients from pursuing refractive surgery.
A RESURGENCE
The second half of 2020 brought a gradual, steady, and welcome increase in the demand for refractive surgery. This increase is currently ongoing.
The implementation of strict guidelines from ophthalmologic societies instilled confidence in surgeons and patients. One major change was a requirement to wash the ocular surface with 0.25% povidone-iodine 10 minutes before refractive surgery. This procedure is virucidal, and no untoward effect on the corneal surface has been reported.
The reaction to the current pandemic has resembled the five stages of grief: denial, anger, bargaining, depression, and acceptance. Humankind has accepted that life must go on and has taken steps toward acclimating to this new normal, including the wearing of face masks. People who depend on glasses for functional vision have had to contend with foggy lenses. This trivial but constant annoyance has motivated some of them to seek vision correction procedures. This combined with two other factors (a delayed case load and a desire among patients to invest in themselves during an unpredictable time) have contributed to a resurgence in refractive surgery.
A FUTURE NEED
COVID-19 forced a major worldwide shift to online avenues of communication. Video conferencing has become ubiquitous, and school-aged children engage in varying amounts of online education. This increased screen time may produce an uptick in the number of adolescents with myopia, which could lead to a surge in demand for refractive surgery in the future.
Reflecting on this pandemic brings to mind the words of the US science fiction author Octavia E. Butler: “In order to rise from its own ashes, a phoenix first must burn.”
US Outlook: Despite the Lockdown, Refractive Practices Are Thriving
Sonia H. Yoo, MD
Miami

In mid-March 2020, because of the growing prevalence of COVID-19 in Miami, elective refractive surgery was suspended at the Bascom Palmer Eye Institute (BPEI), where I practice. This directive was in effect from March 18 to May 18, 2020. When the provision of refractive surgery resumed at our practice, the requirements for proceeding with surgery included patients’ being able to answer no to all COVID screening questions (see COVID-19 Screening Questions) and obtaining a negative COVID-19 polymerase chain reaction nasopharyngeal swab test result 24 to 48 hours before their scheduled surgery (swabs all obtained at BPEI and run through the University of Miami laboratory).1,2
Some of the changes BPEI made in response to the pandemic were offering telehealth screening visits before in-person appointments and spacing out in-person visits to minimize the time patients spent in the hospital and to maintain adequate physical distancing in waiting rooms. BPEI also reduced the price of laser refractive procedures to offset both a possible decrease in their disposable income for elective surgery and the fear we anticipated that patients would feel about coming to the hospital for elective surgery.
The silver lining to this situation is that, since the resumption of refractive services, surgical volume and revenue have outperformed our levels during the same months in 2019. The pandemic prompted us to inadvertently price our services more competitively in our local market. It also propelled us forward in terms of offering telemedicine. We have found that telehealth appointments work well for refractive surgery patients because they often can share their historical prescriptions and tend to appreciate the convenience of consulting with a provider before an in-person visit.
It turns out that many patients are currently seeking refractive surgery because of the inconvenience of glasses that fog up while they are wearing masks. Furthermore, many patients are working from home, so they have greater flexibility to schedule surgery and heal from home, thus decreasing the number of missed workdays.
CONCLUSION
BPEI’s refractive practice has thrived despite the 2-month shutdown. Now that the COVID-19 vaccination process has begun, we anticipate bright days ahead this year for refractive surgery.
COVID-19 SCREENING QUESTIONS
1. Have you had a positive COVID -19 test, or are you awaiting the result of a COVID-19 test?
2. Have you been in close contact with anyone who has COVID-19 or is being tested for COVID-19?
3. Have you experienced a new onset of flu-like symptoms, sore throat, shortness of breath, difficulty breathing, nausea/vomiting, diarrhea, headache, body aches, or lack of smell or taste in the past 3 days?
4. Have you traveled by air or outside the state of Florida within the past 10 days?
1. Fadlallah A, Khattar G, Habre C, Khanafer D. LASIK procedures during COVID-19. J Cataract Refract Surg. 2020;46(12):1682.
2. Zhang J, Aslanides IM, Selimis V, et al. A comprehensive strategy for laser corneal refractive surgery during the COVID-19 epidemic in a tertiary teaching hospital in Wenzhou, China. J Ophthalmol. 2020;2020:4835630.

