

Over the past decade, SMILE has demonstrated safety, efficacy, and stability for the treatment of myopia and myopic astigmatism.1 Patients’ postoperative recovery, in terms of dry eye and corneal sensitivity, has been reported to be better after SMILE compared with LASIK.2,3
Hyperopic SMILE has not yet been approved by the FDA or received the CE Mark, but research shows promise.
INVESTIGATING HYPEROPIC SMILE
The importance of optical zone centration and diameter in corneal laser refractive surgery, especially hyperopic treatments, is well known. My colleagues and I examined optical zone centration in a prospective study of 60 consecutive SMILE procedures performed on hyperopic eyes (1.00–7.00 D; astigmatism, ≤ 6.00 D) and compared these findings to results with LASIK performed using a modern laser with eye-tracking technology (MEL90, Carl Zeiss Meditec).4 We found that the centration with the SMILE fixation system was equivalent to that with the 1,000-Hz tracker on the MEL90, and the SMILE eyes even had a slightly lower mean centration offset than LASIK-treated eyes with the same standard deviation (scatter).
We also analyzed optical zone diameter (Figure) and induced spherical aberration in the same study population.5 Results were compared with matched controls in our hyperopic LASIK database. The mean optical zone used for SMILE was 6.37 mm, with a 2-mm transition zone, and LASIK was performed with 6.5- and 7-mm optical zones. Hyperopic SMILE eyes treated in a 6.3-mm zone produced a mean optical zone diameter larger than that achieved with LASIK using a 6.5-mm optical zone. Hyperopic SMILE and LASIK with a 7-mm optical zone induced similar spherical aberration; however, SMILE was performed in a smaller optical zone.
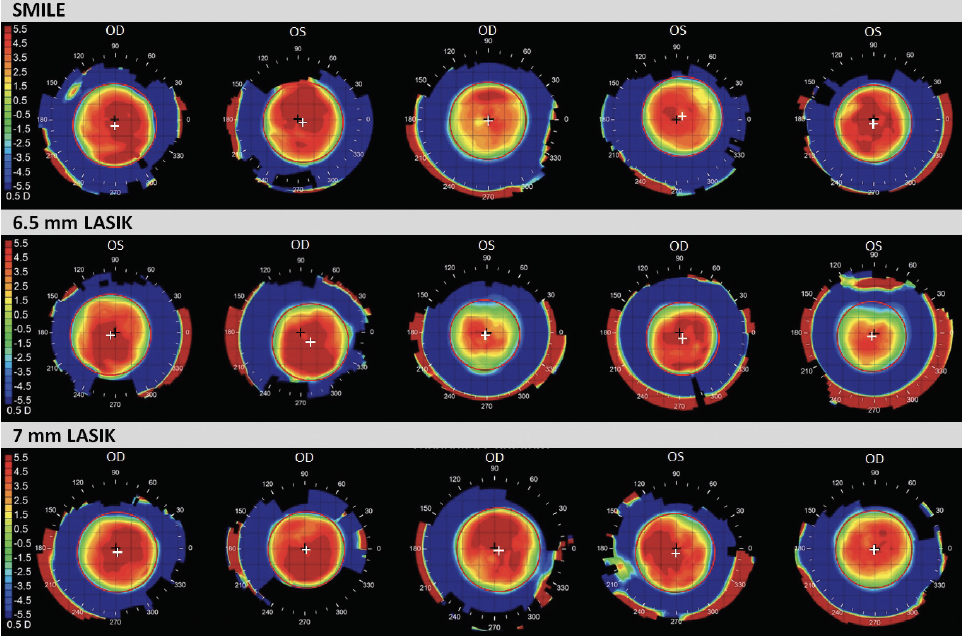
Figure. Examples of Atlas tangential difference maps for SMILE, LASIK with a 6.5-mm optical zone, and LASIK with a 7-mm optical zone. The perimeter of the optical zone is identified by the red circle, the center of the optical zone is indicated by the white cross, and the corneal vertex is indicated by the black cross.
In another study, 93 eyes were treated with hyperopic SMILE (range of attempted spherical equivalent, 1.00–6.90 D; cylinder, up to -3.50 D).6 After 12 months of follow-up, uncorrected distance visual acuity was 20/32 or better in 62% of eyes with a plano target, relative to 62% of eyes with a preoperative corrected distance visual acuity of 20/32 or better. Spherical equivalent relative to target was -0.19 ±0.90 D (range, -2.07 to +3.50 D), and it was within ±0.50 D in 53% of eyes.
LOOKING AHEAD
A multicenter international study of hyperopic SMILE was recently completed, and plans are being made for future commercialization of the procedure. A preliminary analysis shows that SMILE will provide a safe and effective option to correct hyperopia.
1. Blum M, Lauer AS, Kunert KS, Sekundo W. 10-year results of small incision lenticule extraction. J Refract Surg. 2019;35(10):618-623.
2. Cai WT, Liu QY, Ren CD, et al. Dry eye and corneal sensitivity after small incision lenticule extraction and femtosecond laser-assisted in situ keratomileusis: a meta-analysis. Int J Ophthalmol. 2017;10(4):632-638.
3. Shen Z, Shi K, Yu Y, Yu X, Lin Y, Yao K. Small incision lenticule extraction (SMILE) versus femtosecond laser-assisted in situ keratomileusis (FS-LASIK) for myopia: a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158176.
4. Reinstein DZ, Pradhan KR, Carp GI, et al. Small incision lenticule extraction (SMILE) for hyperopia: optical zone centration. J Refract Surg. 2017;33(3):150-156.
5. Reinstein DZ, Pradhan KR, Carp GI, et al. Small incision lenticule extraction (SMILE) for hyperopia: optical zone diameter and spherical aberration induction. J Refract Surg. 2017;33(6):370-376.
6. Pradhan KR, Reinstein DZ, Carp GI, Archer TJ, Dhungana P. Small incision lenticule extraction (SMILE) for hyperopia: 12-month refractive and visual outcomes. J Refract Surg. 2019;35(7):442-450.

