



The surgical correction of presbyopia is an emerging subspecialty of refractive surgery, and for good reason: The most effective way to address a problem is typically at its source. At the Waring Vision Institute, we have dedicated many of the practice’s resources to the research and development of surgical presbyopia-correction technologies, the clinical evaluation and education of patients with presbyopia, and the optimization of practice patterns for this group.
The institute is dedicated to the surgical correction of presbyopia in accordance with the paradigm of surgical vision for a lifetime that my late father, George O. Waring III, MD, described.
DYSFUNCTIONAL LENS SYNDROME
My mentors Daniel S. Durrie, MD, and Jason E. Stahl, MD, are visionaries in their clinical, surgical, and research approaches to presbyopia. During my fellowship training with them, we expanded on the original description of crystalline lens dysfunction set forth by one of the most prolific and productive modern refractive surgeons, Jorge L. Alió, MD, PhD, FEBOphth.1 In 2007, we proposed that the lens’ optical dysfunction is syndromic in nature and includes presbyopia, opacity, and aberrations.2 We subsequently coined the term dysfunctional lens syndrome (DLS) and developed a classification system for it.3
The evolution of this approach to the treatment of patients with DLS of any stage was based on the experiences of patients in their 50s stating that their LASIK had “worn off.” We began to use objective diagnostic instruments to study the impact of the aging crystalline lens—at the time this was commonly referred to as early cataract—on quality of vision. When we considered how many of the patients who chose to undergo LASIK as an alternative to wearing reading glasses or bifocals would later have their crystalline lenses removed, we realized that we should be treating the source of presbyopia (ie, the lens) instead of the cornea.
We have demonstrated in prospective trials that refractive lens exchange (RLE) objectively improves quality of vision3,4—something that corneal laser vision correction (LVC) cannot do in eyes with early lens opacity. In our experience, patient satisfaction also appears to be higher after RLE than blended vision LASIK. We believe this difference in satisfaction is primarily owing to the maintenance of stereopsis after lens replacement and its contribution to depth perception, summed UCVA, and contrast sensitivity.
A DIFFERENT CONVERSATION
Thanks to advances in laser and IOL technologies, surgeons are better equipped now than ever before to address the source of presbyopia. During the preoperative consultation, we explain to patients that LASIK, PRK, SMILE, and phakic IOLs are typically used to address vision problems (ie, refractive error) with which people are born. In contrast, RLE and cataract surgery are performed to address issues related to aging. The former can be performed for the first and second stages of DLS, and cataract surgery is performed for the third stage of DLS (Figure 1). We refer to RLE as custom lens replacement when discussing this option with patients. Further, as part of the educational process, we provide patients with an objective demonstration of how aging can change the crystalline lens.
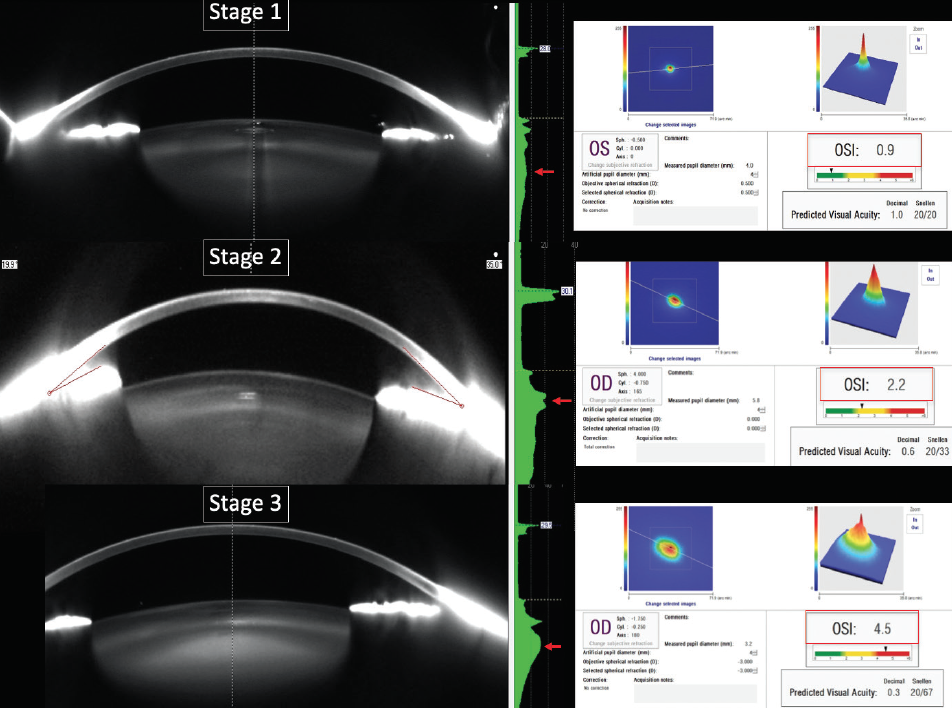
Figure 1. The stages of DLS.
We emphasize that lasers are used to perform both LVC and RLE and that postoperative visual recovery is similar after both types of procedure. We explain that RLE treats the source of the problem; that it can improve both distance and near visual acuity; that it can preserve depth perception; and that, by preventing cataract formation, it obviates the need for LVC or cataract surgery in the future. We carefully outline the potential shortcomings of RLE such as dysphotopsia, a need for reading glasses, opacification of the IOL or capsular bag that may require polishing, and residual refractive error that may require a refractive enhancement or IOL exchange. Risks and benefits are discussed in detail.
PATIENT ACCEPTANCE
Our approach to presbyopia correction has been well accepted by our patients. Based on our outcomes and overall patient satisfaction, we are performing RLE (Figure 2) instead of LVC on an increasing number of individuals with early presbyopia. Risk factors such as high axial myopia are taken into consideration; lens replacement may be deferred, and/or a patient may be referred for a retina consultation.
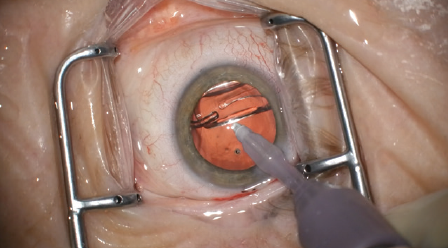
Figure 2. IOL placement during an RLE procedure.
RLE has become one of the fastest-growing segments in our practice,5 and we expect this trend to continue.
1. Alió JL, Schimchak P, Negri HP, Montés-Micó R. Crystalline lens optical dysfunction through aging. Ophthalmology. 2005;112(11):2022-2029.
2. Waring IV GO. Diagnosis and treatment of dysfunctional lens syndrome. Cataract & Refractive Surgery Today. 2013;13(3):36-38.
3. Waring GO IV, Rocha KM. Characterization of the dysfunctional lens syndrome and a review of the literature. Curr Ophthalmol Rep. 2018;6:249-255.
4. Tremblay DM, Waring IV GO, Din HA. Evaluation of improving in forward light scatter and ocular scatter index with double-pass wavefront after dysfunctional lens replacement. Paper presented at: ASCRS/AOA Annual Meeting; April 21, 2015; San Diego.
5. Mercer RN, Milliken CM, Waring GO, Rocha KM. Future trends in presbyopia correction. J Refract Surg. 2021;37(6 suppl):S28-S34.

