

I was fortunate to perform my training, starting in residency, under surgeons like Parag Majmudar, MD, and Jonathan B. Rubenstein, MD, who were mindful of being refractively intelligent in taking care of cataract surgery patients. So from the get-go, I knew that it's not only the cataract surgery that’s important, but the patient’s refractive outcome. I was encouraged, once I felt fairly comfortable in the eye during routine cases, to consider the management of corneal astigmatism.
Even in residency, I carried around a little card in my wallet with the Koch nomogram for corneal astigmatism management with corneal relaxing incisions. I was fortunate to train at the Baylor College of Medicine and learn under absolutely top-notch surgeons, including Douglas D. Koch, MD, and then become his partner, and this was at the top of mind at all times: trying to create a refractively intelligent outcome in my cataract surgeries.
Subsequently, with the approval of toric IOLs, we recognized that some refractive surprises did not just occur because the cornea was different from patient to patient, whether in width, thickness, or hysteresis, but that there was more to corneal astigmatism management. It was exciting learning and working with Dr. Koch on the concept of the role of posterior corneal astigmatism. We saw that, with toric IOLs, many times we were undercorrecting against-the-rule (ATR) astigmatism and flipping with-the-rule (WTR) astigmatism. Why was this happening? We finally figured out that posterior corneal astigmatism was a factor in the outcome (Figure). (Editor’s note: For more information on the role of posterior corneal astigmatism, see Dr. Yeu’s article in MillennialEYE.) Fortunately for all cataract surgeons, the works of Graham D. Barrett, MD, FRANZCO, and Baylor surgeons have continued to help us better understand how the cornea and the lens affect refractive astigmatism (ie, effective lens position, lens tilt).
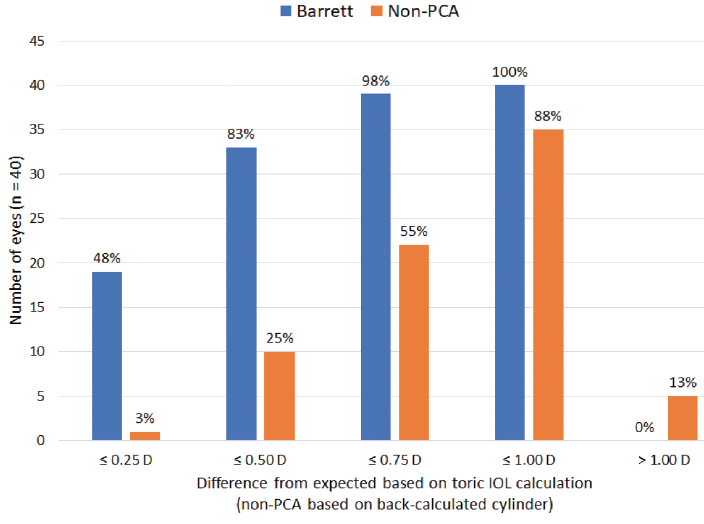
Figure. The difference from expected residual refraction between the Barrett Toric Calculator and a toric calculator that did not include posterior corneal astigmatism.
The past decade has seen the evolution of cataract surgery from assuming that patients will need spectacle correction postoperatively to being as accurate and mindful as possible. We now have fourth-generation formulas that allow us to achieve, given good diagnostics, ±0.50 D of the target in more than 90% of patients. That's an almost LASIK-like level of success.
Presbyopia-correcting lenses add another dimension in our ability to provide patients with excellent outcomes. The recently approved AcrySof IQ PanOptix trifocal IOL (Alcon) is available in a toric version. Certainly, we have to customize surgery for each patient, and we have to understand whether the macula and the cornea can support a 20/20 result. But, that said, it is wonderful that we can provide patients with spectacle independence and meet their needs and desires with our cataract surgery.
I use toric IOLs for eyes with as little as 1.00 D WTR or 0.50 D ATR anterior corneal astigmatism, especially now that Bausch + Lomb offers the lowest cylinder correction with its enVista toric lenses. They can functionally treat as little as 0.80 D of corneal astigmatism. For lower amounts, I offer laser-assisted astigmatic keratotomy.
In the event of postoperative residual error, if the cause is malrotation, I check astigmatismfix.com to see if rotation of the IOL is warranted. If it is not a rotation issue, the solution depends on how much cylinder remains. If it is greater than 1.00 D, I consider an IOL exchange; if less than 1.00 D and the refractive cylinder demonstrates undercorrection and is within the same meridian as the toric alignment, I perform manual limbal relaxing incisions (LRIs), PRK, or LASIK. If the meridian is opposite to the original, I recommend against LRIs, as my own experience has demonstrated suboptimal distance UCVA when the LRIs are in a different meridian from the original toric IOL alignment. These patients seemingly do well with LASIK or PRK, but, again, for more than 1.00 D of residual cylinder, I prefer to exchange the IOL.
TOP TIPS
For those considering beginning to use toric IOLs, I suggest starting with patients with low levels of astigmatism rather than higher levels (1.00–2.00 D) in an eye of average length (23–25 mm). It may be true that patients with 2.50 or 3.00 D of cylinder would be happy just to reduce their overall astigmatism, but remember that, if there is an error in alignment, each degree of error leads to a greater overall impact. Whatever the starting power, every degree you're off target means a 3.3% reduction in the intended astigmatic correction; therefore, misalignment of a higher-power toric lens will have a greater effect than misalignment of a low-power toric lens.
Another tip for beginning with astigmatism management is to start recognizing what real keratometric astigmatism is, as distinct from induced astigmatism. By induced astigmatism, in this context, I mean that ocular surface disease and mechanical disorders such as corneal staining from dry eye disease or anterior corneal dystrophy can distort the ocular surface. Just be careful to note the source of the astigmatism. Look for consistency among your diagnostic instruments, both in magnitude and meridian. If the amount of astigmatism or the average corneal power is different between diagnostics, this may be alerting you to the presence of evaporative dry eye disease. The numbers aren't quite right because the precorneal tear film is not stable.
Find out my preferred IOLs for astigmatism correction in the Table. Click here!

