Proponents of laser cataract surgery have predominantly been drawn to the reproducibility and uniformity of femtosecond laser–created anterior capsulotomies and the laser’s lens fragmentation capabilities. Adoption of laser cataract surgery has, however, been limited by the high costs of acquiring, maintaining, and using the technology.
Because of the added costs, patients generally must pay a premium—out of pocket—to have the procedure. However, this arrangement may be prohibited in many global settings where cataract surgery is covered by the government or by private insurance.
AT A GLANCE
- When used in combination, two disposable technologies can supplant the femtosecond laser in many situations.
- Surgeons can try out and selectively use the Zepto and miLoop devices without the large capital equipment investment that laser cataract surgery entails.
- With the miLoop, it is advised to start with large pupils and master bisecting medium-density nuclei before progressing to brunescent lenses.
A second drawback to laser cataract surgery is its logistical disruption of normal surgical workflow. Precious space within the OR or ambulatory surgery center (ASC) must be allocated for the laser, and the laser steps must be done prior to prepping and draping the eye on the operating table.
The additional costs and surgical inefficiency would be justified if use of the laser provided a consistent and significant improvement in surgical or refractive outcomes or a reduced complication rate. However, the largest studies, including the ESCRS EUREQUO clinical trial,1-3 have failed to demonstrate significant superiority of laser cataract surgery over surgery without the laser.
Cedric Schweitzer, MD, FEBO, presented results from the FEMCAT study at the 2017 ESCRS meeting in Lisbon.4 This is the most important study completed to date because it was a randomized controlled trial in which more than 900 patients underwent either bilateral manual phacoemulsification or bilateral laser cataract surgery. Bias was reduced by two important study features: (1) patients did not pay extra for laser cataract surgery, and (2) manual phaco patients underwent sham docking so that they did not know whether they had the laser treatment or not. Overall safety, visual, and refractive outcomes were similar in both groups, indicating that laser cataract surgery was neither superior nor inferior to phaco.
Studies notwithstanding, cataract surgery is a complex craft, and surgeons understandably develop individual preferences for different techniques and instrumentation. There are two newly approved disposable technologies that may interest surgeons desiring some of the advantages of laser cataract surgery without the cost and workflow disruption involved in incorporating the femtosecond laser.
ALTERNATIVE FOR AUTOMATED CAPSULOTOMY
Background. In June 2017, the FDA issued regulatory clearance for the »Zepto device (Mynosys), a handheld technology designed to create a precise capsulotomy using a method the company calls precision pulse capsulotomy (PPC).5,6 As with laser-created capsulotomy, Zepto PPC is intended to reproducibly automate the procedure and ensure a perfectly sized, round capsulotomy.
The procedure is performed with a disposable instrument that is inserted instead of capsulorrhexis forceps in the conventional surgical sequence after the anterior chamber has been filled with an OVD (Figure 1, top left). It therefore avoids the workflow challenges and increased procedural time necessitated for laser use.
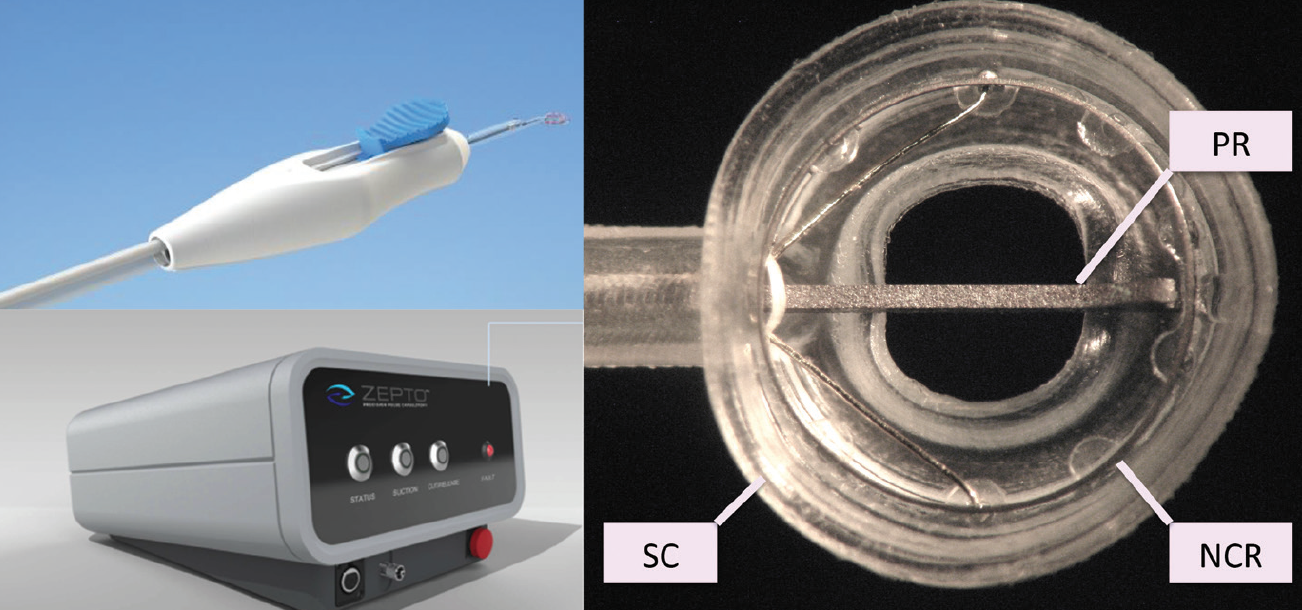
Figure 1. Zepto capsulotomy instrumentation: Disposable handpiece with blue slider to extend and retract the metal push rod (top left); portable console that powers suction and cutting functions (bottom left); close-up view of undersurface of the Zepto tip (right); the retractable push rod (PR) is extended to narrow the profile of the nitinol cutting ring (NCR) and the surrounding silicone cover (SC).
How it works. A small console powers the disposable handpiece and capsulotomy tip (Figure 1, bottom left). The cutting element is a nitinol ring with a precisely engineered micrometer edge that creates a capsulotomy 5.2 mm in diameter. Nitinol is a superelastic shape-memory alloy; it can be deformed or compressed and will rebound to its original shape. A thin, transparent silicone suction cup shell surrounding the nitinol ring is stretched and elongated with a metal push rod to facilitate insertion through a 2.2-mm clear corneal incision (CCI; Figure 1, right). The Zepto tip reassumes the original shape once it is opened inside the anterior chamber by withdrawing the push rod.
Suction is fundamental to how Zepto works. The suction line is primed with balanced salt solution prior to surgery, creating an efficient hydraulic suction system. This ensures even and complete apposition of the bottom of the nitinol ring to the capsule to create a unique, strong capsulotomy edge. Only a slight amount of suction is needed to temporarily remove a small amount of OVD under the suction cup to appose the anterior capsule against the bottom edge of the nitinol ring, which has been precisely engineered at the micron scale to enable uniform cutting of the capsule. The silicone suction cup has a clear central opening that permits the patient to fixate on the microscope light filament during positioning of the device. The surgeon positions the ring and surrounding silicone suction cup on the anterior capsular surface in the desired capsulotomy location prior to applying a small amount of suction via the external console that is operated by the circulating nurse.
A series of rapid electrical micropulses then creates just enough heat to vaporize water molecules trapped between the anterior capsule and the nitinol ring. The phase transition happens so quickly (approximately 4 msec) that there is a simultaneous circumferential mechanical cleavage of the anterior capsule. The result is a complete circular and perfectly sized capsulotomy with no tags and without any tissue coagulation such as would occur with cautery.
The device is then floated off the capsule by the release of OVD, which was previously temporarily evacuated from the suction cup to produce apposition of the nitinol ring to the capsule. Once it is floated off, the device is withdrawn through the incision, and the surgeon proceeds with hydrodissection and phacoemulsification.
Recent modifications. Collateral safety of ocular tissue is achieved through two design features. First, the application of energy is extremely brief and confined only to the microscopic edge of the nitinol ring. Second, during activation, the nitinol ring is completely covered by the silicone suction cup and further insulated by the surrounding OVD.
Modifications in the manufacturing of the nitinol cutting ring have recently been made. The new method, called chemical vapor deposition (CVD), literally builds the nitinol ring molecule by molecule and allows incredibly tight tolerances in the manufacturing process, down to the 1-µm level. Use of CVD technology in the Zepto cutting element has yielded consistent and, more important, stronger capsulotomies compared with first-generation devices. This modification should significantly improve the cutting consistency of the technology.
Applications for Zepto. Because it is an integrated step during conventional phacoemulsification, PPC can be performed after insertion of iris expansion devices for small pupils. For eyes with a poor red reflex, PPC does not require capsular staining. This feature is useful for white cataracts, brunescent lenses, and those with diffuse anterior cortical spokes. The lower cost of the device relative to the femtosecond laser ideally will allow surgeons to make PPC available to all patients independent of affordability and regional regulations regarding balance billing.
As with laser cataract surgery, some surgeons may specifically use Zepto PPC only for complicated cases, much as they would use trypan blue dye, pupil expansion rings, or capsular tension rings. Others may value the perfectly circular and precise capsulotomy dimensions for premium refractive IOL implantation (Figure 2). In this context, Zepto PPC may provide a less expensive and more efficient adjunct than the femtosecond laser. The ability to center the capsulotomy on the visual axis as the patient fixates on the microscope light through the central window may be advantageous for diffractive extended depth of focus and multifocal IOLs.
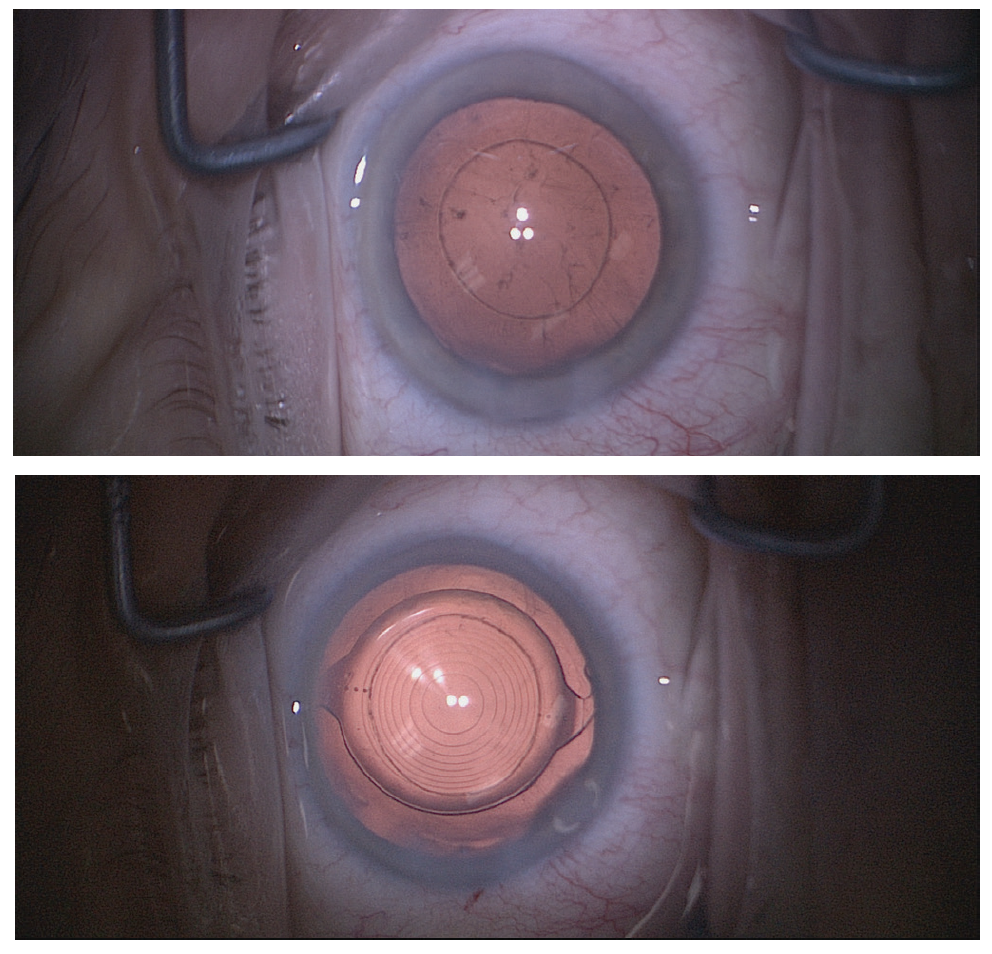
Figure 2. Zepto capsulotomy following cortical cleanup (top) and implantation of a Symfony extended depth of focus IOL (Johnson & Johnson Vision; bottom).
Finally, some cataract surgeons may be tempted to use the device routinely on every case, particularly if it is on average faster and more consistent than manual capsulorrhexis. The beauty of a disposable instrument is the versatility it provides to surgeons without the economic pressures and commitment of purchasing a femtosecond laser or the need for patients to pay extra for the technology.
ALTERNATIVE FOR NUCLEAR FRAGMENTATION
Background. The handheld, disposable »miLoop Lens Fragmentation Device (Iantech) is used to manually fragment the nucleus within the capsular bag. This device, which has received FDA regulatory clearance, incorporates a thin memory-shaped filament loop, made, like the Zepto, of the alloy nitinol.
How it works. The nitinol loop is used to encircle the nucleus following capsulotomy and hydrodissection. Using a manual slider on the handpiece, the loop is constricted like a wire snare to bisect the nucleus into two heminuclei.
The superelastic property of nitinol allows contraction of the loop to a radius of 1.5 mm so that it can pass through a small CCI (Figure 3, top). It is then opened and expanded to a radius of 10.5 mm just beneath the anterior capsule in the coronal plane (Figure 3, second from top). Once the loop is completely expanded, it is swept within the capsular bag along the hydrodissection plane against the internal capsular contour so that it completely encircles the nucleus in the sagittal plane. At this point, the handpiece slider is used to constrict the loop back to its smallest 1.5 mm radius. The nitinol filament transects the nucleus, essentially cheesewiring through a nucleus of any density using purely manual energy directed centripetally. After rotating the nucleus 90°, these steps are repeated to create quadrants before the phaco tip is introduced. The 300 µm–diameter nitinol loop is smooth and curved so as to minimize deformation of the surrounding capsular bag during expansion and placement.
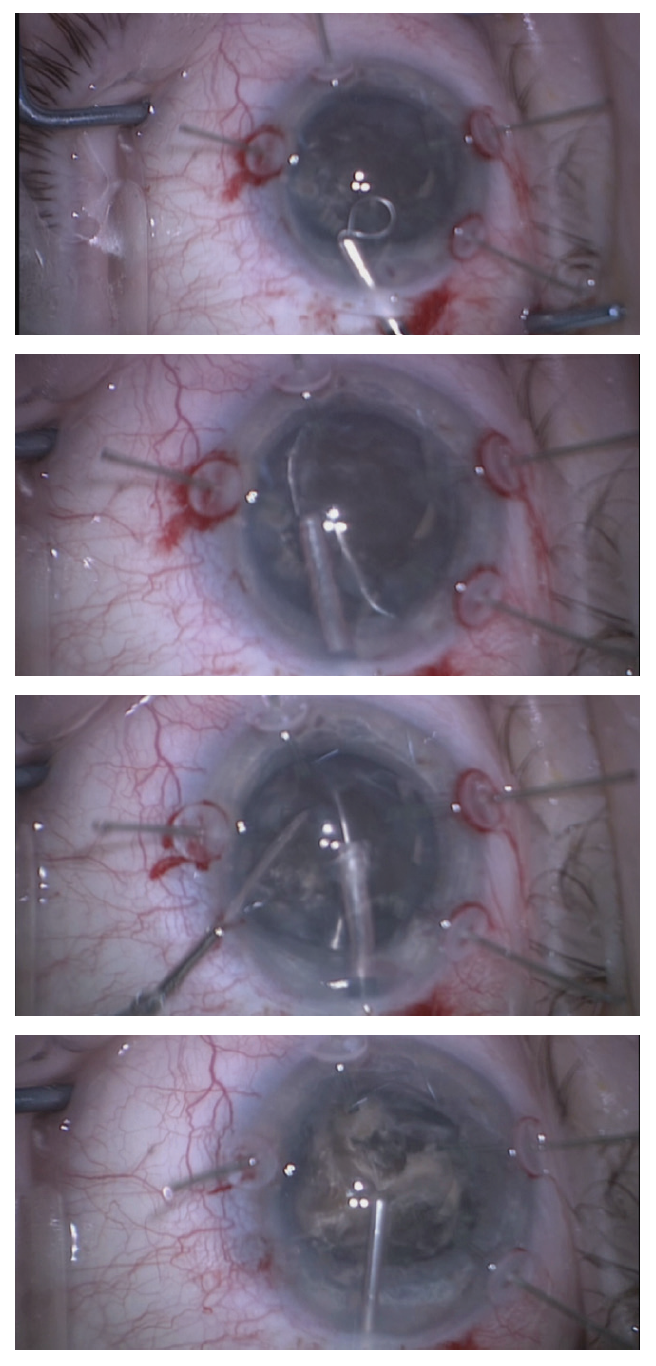
Figure 3. miLoop fragmentation of a rock-hard nucleus. The loop is contracted to the smallest diameter (top) to pass through a clear corneal incision. It is expanded to its full diameter in the coronal plane beneath the anterior capsule (second from top). Once the loop is positioned in the sagittal plane, a second instrument applies counterpressure to the nasal nuclear pole prior to initiating the cutting (third from top). After two cuts, the brunescent nucleus has been manually divided into four quadrants. The cruciate pattern of the two full-thickness cuts is evident after injecting OVD (bottom).
Applications for miLoop. Surgeons who are not adept at phaco chop may consider using the miLoop as a prechopping tool. One of its most attractive and obvious applications, however, is for manually fragmenting a brunescent nucleus. Because of the increased nuclear thickness and the absence of epinucleus in these lenses, phaco chop frequently fails to divide the leathery posterior nuclear plate. The femtosecond laser is also unable to transect this posterior nuclear plate because of its proximity to the posterior capsule. The miLoop will always fully transect the nucleus because the soft, thin nitinol filament completely encircles the nucleus before cutting it.
For dense nuclei, constricting the filament tends to tilt the nasal pole of the nucleus forward, to the point of prolapsing it through the capsulotomy. Therefore, a second instrument should be used to provide counterpressure against the nasal nuclear pole (Figure 3, third from top). This allows the nitinol filament to complete its cutting path without excessive nuclear displacement and zonular stress. I frequently use the miLoop just to bisect a brunescent nucleus and then start vertical chopping of each heminucleus. Others might choose to spend the additional time to cut the nucleus into quadrants (Figure 3, bottom).
LEARNING CURVES
Both the Zepto and miLoop devices have a learning curve, but it is relatively short in each instance. Start with large pupils and master bisecting medium-density nuclei with the miLoop before progressing to brunescent lenses.
We now have two disposable technologies in our armamentarium that, in combination, can supplant the femtosecond laser in many situations. Fortunately, surgeons can try out and selectively use these instruments without the large capital equipment investment that laser cataract surgery entails.
1. Day AC, Gore DM, Bunce C, Evans JR. Laser-assisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery. Cochrane Database Syst Rev. 2016;7:CD010735.
2. Popovic M, Campos-Moller X, Schlenker MB, Ahmed IIK. Efficacy and safety of femtosecond laser-assisted cataract surgery compared with manual cataract surgery: A meta-analysis of 14567 eyes. Ophthalmology. 2016; 123: 2113-2126.
3. Manning S, Barry P, Henry Y, et al. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: Study from the European Registry of Quality Outcomes for Cataract and Refractive Surgery. J Cataract Refract Surg. 2016;42:1779-1790.
4. Schweitzer C. Six years on: Is FLACS a better and safer operation than phaco?:
Evidence from the French FEMCAT study. Paper presented at: the 2017 ESCRS Annual Meeting; October 7-11, 2017; Lisbon, Portugal.
5. Chang DF, Mamalis N, Werner L. Precision pulse capsulotomy – Preclinical safety and performance of a new capsulotomy technology. Ophthalmology. 2016;123:255-264.
6. Thompson VM, Berdahl JP, Solano JM, Chang DF. Comparison of manual, femtosecond laser, and precision pulse capsulotomy edge tear in paired human cadaver eyes. Ophthalmology. 2016;123:265-274.