

We have all read news stories heralding the dawn of telemedicine and predicting that, soon, patients will receive the bulk of their health care through connected body sensors and ever-present digital “providers.” Speaking as a patient, I am thankful this revolution has not yet occurred, but a few startups have recently arisen to digitize, and possibly supersede, in-office phoropter-based refraction. Why have they sought to do this? Mostly, they wish to unlock the multibillion dollar US eyewear market, whose prescriptions have, until now, exclusively originated from the refracting lanes of about 20,000 ophthalmologists and 35,000 optometrists.
AT A GLANCE
• Several startups have recently arisen to digitize, and possibly supersede, in-office phoropter-based refraction.
• In underserved populations or developing nations, some of these lower-cost technologies may have a role. On the other hand, discerning, 18- to 45-year-old patients in first-world nations may not tolerate measurements that are off by 0.50 or 1.00 D.
• As these companies market their services to consumers, optometrists and ophthalmologists will have to educate their patients on the importance of comprehensive anatomic eye examinations to screen for disease.
This article highlights some of the new eye care telehealth startups and their approach to telerefraction. Until state laws change, these companies must have their digital prescriptions “signed” by licensed eye care providers (MD, DO, or OD), who do so remotely. It is therefore not surprising that, like consumer tech companies that are disrupting other industries (eg, Uber and Airbnb), these startups have begun wooing state legislatures.
THE EARLY CONTENDERS
Opternative
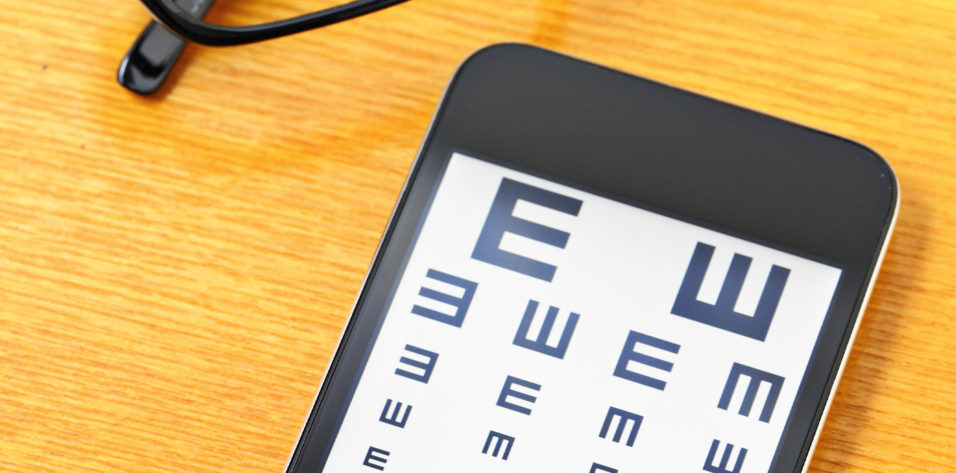
This is the original (and still controversial) online self-refracting technology (Figure 1). It promises an accurate at-home refraction with just a computer, a smartphone, and 12 feet of walking space. Opternative charges $40 for a glasses or contact lens prescription or $60 for both.

Figure 1. Opternative promises accurate at-home refraction with a computer and smartphone.
I tried this service and found the result to be close but not perfect. First, users enter their shoe size, after which they are instructed to walk a specified number of steps from the computer. Users are shown dozens of lines on the screen and asked via visual and voice prompts to respond using a paired smartphone as a touchscreen remote. The process is laborious and repetitive and took me approximately 25 minutes to complete. Afterward, the user waits about 24 hours for an Opternative ophthalmologist (as of this writing, the company claims to have partnered with licensed ophthalmologists in 39 states) to officially provide the prescription.
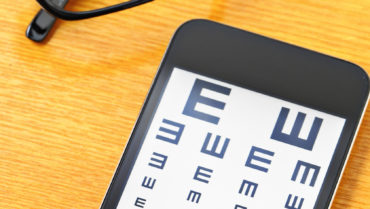
Figure 2 compares the online testing results to a phoropter refraction, according to an Opternative-sponsored study.1 In my opinion, variability is too significant for the typical millennial patient—Opternative limits the test to people aged 18 to 50 years without presbyopia—but this automated technology can allow those without access to traditional eye care to obtain glasses.
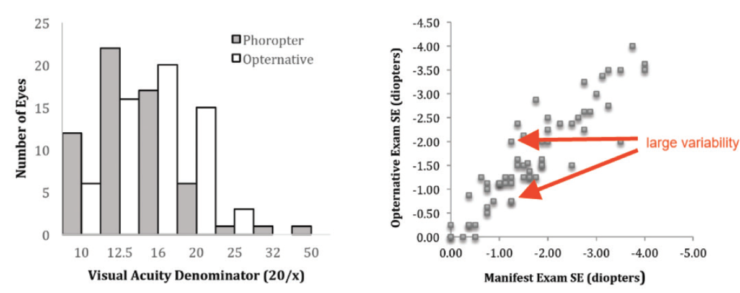
Figure 2. Opternative’s online testing results compared to a phoropter refraction.
Simple Contacts
This new startup is the simplest of all: it allows patients to reorder their contact lenses without having to undergo an in-office eye exam. The founders estimate that 80% of contact lens reorders have no change in prescription, so this app simply “verifies” the patient’s good vision with his or her contacts in.
Using the smartphone app, users check off boxes confirming that they have had a dilated eye exam in the past 4 years and that they do not have a host of other eye diseases. Then, they are prompted to walk 10 feet away from their phone and read the displayed letters (Figure 3). Video and voice of the user are recorded and sent to a remote ophthalmologist for review and a renewal of the patient’s current self-reported contact lens prescription. Simple Contacts currently charges $10 for the service and requires users to order their contacts from the Simple Contacts site, which offers all the popular brands at standard prices. I tried this service, and it was very simple. If someone really wanted to reorder contact lenses, however, he or she could easily find a way to “pass” the app’s test, no matter his or her vision.
Figure 3. Simple Contacts tests vision on a smartphone.
EyeNetra
EyeNetra has developed a smartphone-based subjective “autorefractor” that allows a patient to perform a self-refraction using what looks like a cross between a ViewMaster (Mattel) and a virtual reality headset (Figure 4). I tried the service at a trade show, and it took a few minutes to complete testing of each eye. Users hold and look through the device as they would a pair of binoculars (Figure 5). It is attached to a Samsung smartphone that cues users through visual and audible prompts to press one of two buttons to align two shapes. The process is repeated about 18 times. A digital refraction is then provided. Studies show the results compare well with those obtained with a traditional autorefractor.2

Figure 4. EyeNetra’s smartphone-based subjective autorefractor.

Figure 5. Users hold the EyeNetra device to perform self-refraction.
Currently, the company sells the device to providers for $1,099 (with an option to buy a separate and nifty portable phoropter and smartphone-based lensometer). EyeNetra had a telehealth service, Blink, where technicians (not doctors) made house calls with these devices, and ophthalmologists later remotely signed prescriptions, but it seems to have gone offline for now. The company now offers a service, OnSight, where optometrists are dispatched to corporate locations to conduct on-site refractions.
SmartVision Labs
This is a compact and portable smartphone-based autorefractor (the unit is built around a specially configured iPhone [Apple]). Using a portable aberrometer, the iPhone camera, and lots of computation, the device is able to deliver an objective autorefraction in a few seconds.
I have tried the SVOne Pro in my office, and it works quite well for straightforward cases. The device is placed on a tripod stand and uses audible prompts to guide a patient through a self-autorefraction (Figure 6). When pathology is present, the result can be grossly off, as many traditional autorefractors would be.

Figure 6. SmartVision Labs’ SVOne Pro works well for straightforward cases.

Figure 7. The EyeQue mini scope is temporarily secured to a smartphone.
SmartVision sells the device for $4,750 on its website, but the company’s growing focus is on providing telerefraction services to optical shops that do not have an in-house doctor. Dozens of New York City optical shops have recently placed the units, which send off the autorefractions (and the patient’s visual acuity) to an affiliated ophthalmologist for review and a remotely signed glasses prescription. Without a subjective component, autorefractors are hit or miss, and I am curious to see how this technology will do with discerning patients.
EyeQue
The newest remote refraction technology was initiated by a Kickstarter campaign. The small, $30 device is a mini scope that is temporarily secured to an Android or iPhone and directs a patient to perform a self-refraction (seemingly similar to EyeNetra) by tapping + or - to move two cylinders until they overlap (Figure 7). The process is accomplished in each eye in nine different meridians, generating a refraction. The app allows users to check their refraction repeatedly and chart their changing prescription. EyeQue has presented one study on its website that compares the scope to a Topcon Autorefractor.3 The company reports that the EyeQue was within 0.50 D of the Topcon result 74% of the time.
Summary
Many of the technologies I have described certainly can generate a “pretty good” refraction but seemingly with a substantial standard deviation. Certainly, in underserved populations or developing nations, some of these lower-cost technologies may have a role. On the other hand, many of these companies target the first-world, discerning, 18- to 45-year-old patients, and measurements off by 0.50 or 1.00 D will not be tolerated or, worse, will be detrimental to patients’ eye health.
As these companies market their services to consumers, optometrists and ophthalmologists will have to educate their patients on the importance of comprehensive anatomic eye examinations to screen for disease. Furthermore, eye care providers should become familiar with the strengths and shortcomings of these technologies so that they can continue to deliver high-quality, personalized care and outstanding outcomes to patients—with whichever product allows that.
1. Dow CT. Clinical Trial Summary Report. https://www.opternative.com/clinical-study. Accessed February 14, 2017.
2. Pamplona VF, Trupin S, Cuadros J Modi R. Validation of confidence levels for a cell phone-based refractor (NETRA-G). IOVS. 2015;56:2201.
3. Eyeque. Comparison of the Eyeque Personal Vision Tracker With the Topcon KR-800 Autorefractor. Summary of White Paper. https://www.eyeque.com/scientific_study. October 7, 2016. Accessed February 14, 2017.

