
Kerry D. Solomon, MD: Thank you to everyone for being here today. Our discussion will revolve around identifying common patient expectations and how they’ve changed with the advent of refractive cataract surgery. We’re also going to talk about the innovations that are available today that can help us to increase the accuracy of our outcomes after cataract surgery. It will include preoperative assessments, intraoperative assessments, keratometry (K) measurements, and measurements of not only the anterior and the posterior segment but also the anterior and posterior cornea. Lastly, we will discuss intraoperative innovations for data transfer and alignment accuracy.
LET’S TALK PATIENT EXPECTATIONS
Dr. Solomon: So, with the first question, please also introduce yourself and your practice. My practice, which is located in Charleston, South Carolina, specializes in cataract and refractive surgery. I’ll throw out the first question to Dr. Yeu. What are the refractive expectations of today’s cataract patient?
Elizabeth Yeu, MD: I practice at Virginia Eye Consultants in Virginia, and we are a multispecialty practice. The most important piece of advice I can give to any cataract surgeon is that you must take the time to really recognize who you are serving. In other words, who is your patient base? For us, a lot of our referrals, about 75% of them, do come from our optometric network. We have some optometrists in-house, but they really focus on primary medical care, and therefore we work very closely with them on our patient follow-ups and perioperative care. With that being said, because so much of our network, our surgical volume, and our patient base comes from our OD network, it is so important that we meet patient expectations and provide patients with the outcomes they are looking for because, ultimately, we may only meet these patients three times—once preoperatively and two times during surgery. Everything else, in terms of the functional outcomes and satisfaction, is incumbent upon us to achieve and do everything we can so that our referring doctors keep referring patients to us.
Steven C. Schallhorn, MD: I’m the Chief Medical Officer for Zeiss, and I also practice at Gordon Schanzlin New Vision Institute in La Jolla, California. The expectations of patients who undergo cataract procedures today is going in one direction, and that’s increasing. We’re the victims of our own success: the more successful we are, the more patients expect success. To help match these ever-increasing expectations, we need to continually offer the best available technology and the most appropriate procedures, and we must provide the best patient care. The better we do this today, the better we’re going to have to do it in the future.
John A. Vukich, MD: I specialize in cataract and refractive surgery at Davis Duehr Dean Center for Refractive Surgery in Madison, Wisconsin. We’ve seen an evolution of patients’ visual expectations following cataract surgery. It started maybe 3 decades ago when the ability to more accurately select the implant power became an important factor. Now, we not only remove the cataract, we also have a very specific targeted postoperative refraction. All of our patients have a postoperative refractive expectation.
There is no doubt that we have to meet that demand for refractive accuracy because it drives two things: first, it drives patient expectations, and second, it drives patient satisfaction. It’s part of the world we live in; we want to be able to see the best that we can so that we can participate in the things we like to do. We don’t want to feel old or inhibited by our vision. If we can provide that freedom from glasses, I think we’re doing our patients a great service.
Vance Thompson, MD, FACS: I practice at Vance Thompson Vision in Sioux Falls, South Dakota. My partners and I specialize in cataract and refractive surgery. My partners also specialize in glaucoma, corneal surgery, and aesthetics. I am honored to be here, and this discussion is bound to be both interesting and stimulating.
Historically, I feel like LASIK patients are usually surprised when they lose something with their reading vision after they had surgery. They felt like, in a sense, it wore off. And I feel the opposite with cataract surgery patients; a lot of them don’t really realize they can gain that something back. And so, these cataract surgery patients come in with somewhat lower expectations than LASIK patients do, but once you give them all their options, if you don’t deliver, you’re going to find that their expectations for cataract surgery outcomes were actually quite high.
In order to achieve this, it is imperative that you are diligent with educating patients preoperatively, so that they understand what the technology will do and what it won’t do. What’s been amazing in my practice is that we give patients with lenticular aging the information they need to understand that the lessening of their reading ability is related to the same exact cloudy little lens that we’re about to replace. With that, the light bulb kind of goes off. And so, I tell them we can fix one issue—the clarity—with a monofocal IOL, and they can wear bifocals for the reading vision, or we can fix two issues—the clarity and the reading ability—by using a premium lens technology. I continue to say that the latter solution will give them the near vision of someone in their mid-30s, if we’re going for 20/20 uncorrected, and the former, the monofocal IOL, will give them the near vision of someone who’s 65 to 70 years old if also going for a plano result. But glasses can work great for near. And so, once I set those expectations, that’s when patient expectations go up—when they realize, based on my words, what they can have. The better we educate them, the higher their expectations are, so we have to deliver on those expectations.
Ehsan Sadri, MD, FACS, FAAO: I agree with you, Dr. Thompson. I practice at Atlantis Eyecare, in Newport Beach, California. We are a multispecialty practice that focuses on cornea, glaucoma, pediatric surgery, and oculoplastics. We’re heavily focused on innovative technologies that provide the best care for patients, both anterior segment and posterior segment. I think the most important variable in getting the best outcomes for our patients is the preoperative evaluation and assessment. When done well, it will minimize the number of postoperative surprises that occur. We know we cannot eliminate our postoperative surprises, but we can reduce them by using the right tools and technologies to nail that preoperative assessment, including K measurements, posterior corneal evaluations, and managing the ocular surface before any cataract and refractive surgery procedure takes place.
And I think the biggest thing that we can focus on is getting to know your patient. It sounds so basic, but it’s like free throws, right? Free throws are fundamental in basketball, and if you look at all the fundamental, foundational success in cataract surgery, it comes back to getting to know the patient and his or her specific needs and educating the patient on what technologies will and will not work for him or her.
Dr. Solomon: You know, some of my happiest cataract patients are the ones who come in day 1 or week 1 postoperative saying, “Oh, my God! I can see the leaves on the trees! And I can see such detail that I haven’t seen in years. I can’t remember what it’s like not having to wear glasses.” I think that’s what patients want, but at the end of the day, if we’re charging patients for these services, then it’s upon us to deliver. If we don’t, then I think that’s when patients sometimes can have problems and become unhappy postoperatively.
Now, even with the best of circumstances, we still need enhancement strategies—we can talk about that later—but in general, most of the time, we ought to be able to hit the patient’s expectations. Dr. Vukich, in your practice, what tools are crucial to accomplish the goal the patient wants? Let’s say it’s that they want to see better without glasses. It can be distance or distance and near, it doesn’t matter, but what tools are essential in your practice?
Dr. Vukich: All of our patients are paying something. Typically there is a copay, which in some cases can be substantial. Now we’re offering patients the option to upgrade for advanced technology, which comes with even greater expectations.
There are a couple of things that have really changed my practice. One of them is the ability to reproducibly obtain accurate axial lengths with optical biometry. Second has been the improvement in IOL calculation formulas. The Hill-RBF calculator and the Barrett II formula have revolutionized IOL power accuracy. We currently use CALLISTO eye (Carl Zeiss Meditec) for all of our toric IOL patients (Figure 1). We also use it to project a template to guide our capsulotomies. I’m relying on technology to help me be a better surgeon. Advanced technology is what allows me to deliver exceptional results for my patients.
Figure 1. Markerless reference image with CALLISTO eye to aid in toric IOL alignment.
Image courtesy of Richard S. Davidson, MD
Dr. Solomon: Dr. Yeu, are you doing anything in addition to what Dr. Vukich mentioned?
Dr. Yeu: His points are excellent. First and foremost, we have to listen to our patients, right? We have to learn about their history and what their actual needs are. Seven or 8 years ago, I never thought about how important the patient needs assessment truly was. At that time, I felt that the quality of the technology available for presbyopia correction didn’t suit a lot of patients, simply because we couldn’t correct any more than 0.75 D of astigmatism. Now, it’s a different realm, and some of my happiest patients are the ones for whom you are restoring functional capacity and range of vision—and they’re not the ones who can use glasses. They are the ones who have a greater fall risk, some level of dementia, or Parkinson disease, for instance. We’re thinking about it in a completely different realm now because we do have technologies that are really at a level above and beyond what we could offer patients just a few short years ago.
With that being said, the decision process starts with the patient history and understanding them—what they do, what they want to do, what is important to them. But secondly, especially for toricity correction and astigmatism correction, what we understand about the posterior cornea and having better access to at least the orientation of what is going on posteriorly, coupled with the information we have from the Barrett Toric Calculator, that really helps us hone in on that refractive correction. Any residual astigmatism can lead to issues with their functional vision, and now we have better tools to avoid this from occurring.
LOOKING POSTERIORLY
Dr. Solomon: So, how are you quantifying posterior astigmatism?
Dr. Yeu: I have direct access by utilizing the Cassini LED-based topographer (i-Optics), and I look at the orientation that it provides. I find this tool to be very insightful. Now, regarding the raw number, I still use Koch’s methodology,1 which is this: 83% of patients are aligned with-the-rule (WTR) in the posterior surface of the cornea, which functionally acts like refractive against-the-rule (ATR) astigmatism because the posterior cornea behaves like a negative lens. And we understand, for the most part, with a toric IOL, you must bump down 0.50 D for patients who have WTR astigmatism or bump up 0.50 D for patients who have ATR astigmatism—this is a lot easier when you actually use the toric algorithm. But still, work needs to be done.
The reason we need better technology with direct access to what is going on with the posterior curvature is to truly understand the exact amount of the posterior corneal astigmatism. While the average value of posterior corneal curvature is between 0.30 to 0.40 D WTR, the range is vast and more unpredictable in patients with higher amounts of anterior WTR astigmatism. Also, we really don’t know a whole lot about corneas with oblique astigmatism. We think that patients with this type of astigmatism are WTRs going ATR. In my own personal experience with the Cassini, I believe that there are patients in which naturally occurring oblique astigmatism does exist about half of the time, as a lot of these oblique astigmats also have obliquely-oriented posterior corneal astigmatism about 50% of the time. The Baylor Toric nomogram and the Barrett Toric Calculator provide little insight regarding the posterior corneal contribution is those with anterior oblique corneal astigmatism.
Dr. Solomon: Some of the biometers, such as the IOL Master 700 (Carl Zeiss Meditec), will allow us to look at the posterior cornea in the future. Is that right, Dr. Vukich?
Dr. Vukich: Absolutely. And even beyond that, what we’re looking at is integration of the IOL Master 700 with a real-time image that can be transposed onto the OPMI Lumera microscope (Carl Zeiss Meditec) and the CALLISTO eye. Our data are directly transmitted from the IOL Master 700 to our operating suites. This eliminates the potential for transcription errors. The Barrett II formula is resident on the IOL Master 700, and that saves yet another step. We have found this integration to be much easier for the technicians. In return, it is easier for me have confidence in our IOL selection.
Dr. Schallhorn: I’d just like to go back for a second, something Dr. Vukich talked about earlier, and that is the value of accurate biometry. That really drives the IOL power formulas that ultimately determines the refractive accuracy of our outcomes. Biometry needs to be repeatable and reliable with assurance that the patient is properly fixating. Accurate biometry has many facets, and one example is the contribution of the posterior cornea to the overall optical power of the cornea. Until recently, this has been estimated. We now know that this estimation can result in significant IOL power errors, especially for the amount of astigmatism in toric lenses. This estimation could be greatly improved by directly measuring the curvature of the posterior cornea and including the total corneal power in the new IOL formula. The measurement of the posterior cornea will be incorporated into the IOL Master 700 very soon.
Accurately assessing the shape, structure, and optical properties of the eye (ie, biometry) is foundational to improving the outcomes of cataract procedures (Figures 2 and 3).

Figure 2. The IOL Master 700 versus a nontelecentric biometer.
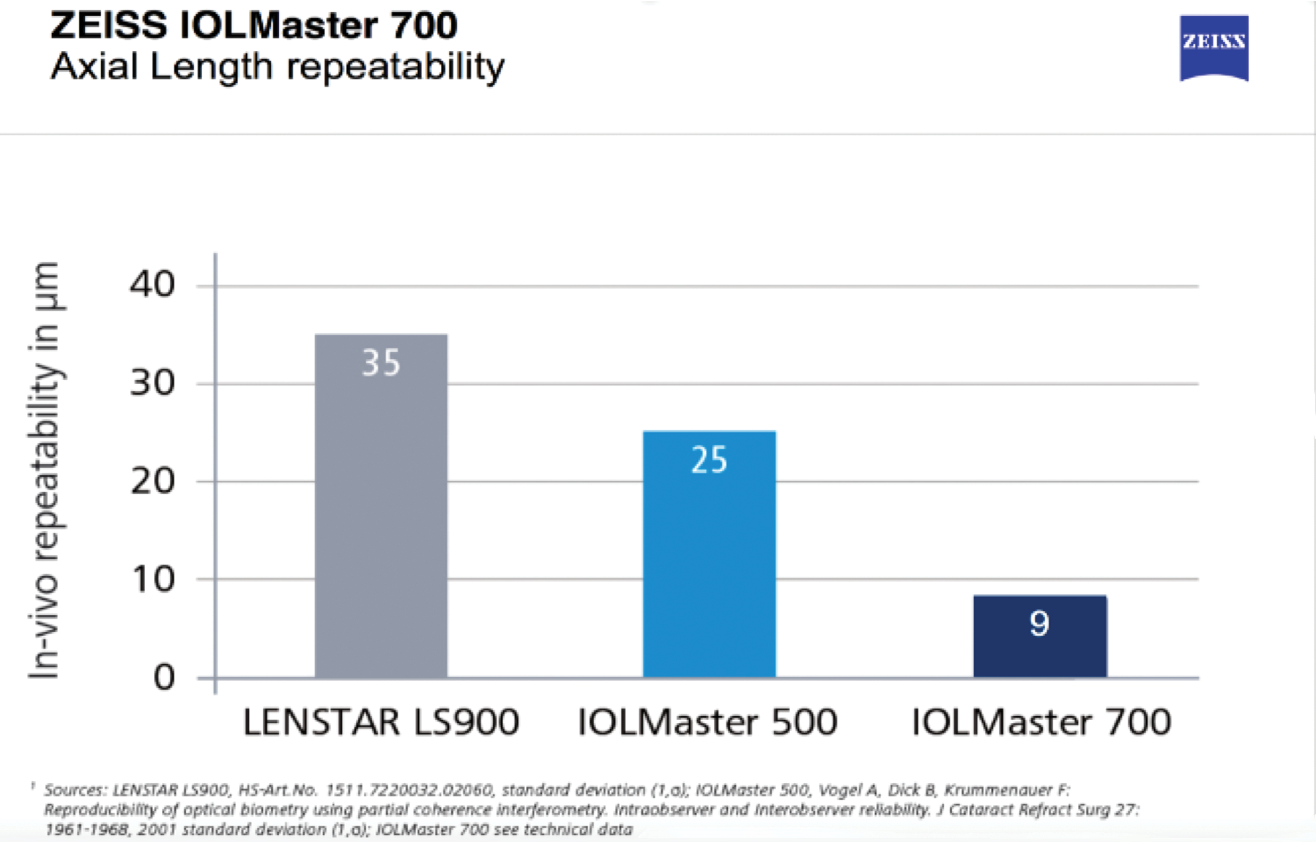
Figure 3. The accuracy of the IOL Master 700 versus the IOL Master 500 versus the Lenstar.
Dr. Solomon: You’re 100% right. And, you know, when I get patients sent to me with an IOL surprise, the first thing I do is repeat the biometry and look at their biometry; 90% of the time, it’s just a bad test or a bad measurement.
One of the nice things about the IOL Master 700 is the optical coherence tomography’s (OCT) capability to measure anterior and posterior surfaces of the cornea. So, you can not only get better K measurements—and posterior measurements in the near future—you can also get total corneal power, which is what you were talking about, Dr. Schallhorn. And the other nice feature that I think is impressive is that you can use the OCT feature not only as a screening tool, but also as a checks and balances to make sure that you’re actually on the macula and that the patient is fixating where they need to fixate. Because, again, garbage in equals garbage out. If you get a bad measurement, that tends to lead to an IOL surprise and a refractive surprise. And more times than not, you’re right. It’s the biometer that’s the problem.
Dr. Schallhorn: The critical component.
Dr. Solomon: Yes.
THE POWER OF SWEPT-SOURCE
Dr. Schallhorn: Another feature of the IOL Master 700 is that it incorporates swept-source OCT. This new and powerful technology allows better penetration into the eye, through even dense cataracts (Figure 4).
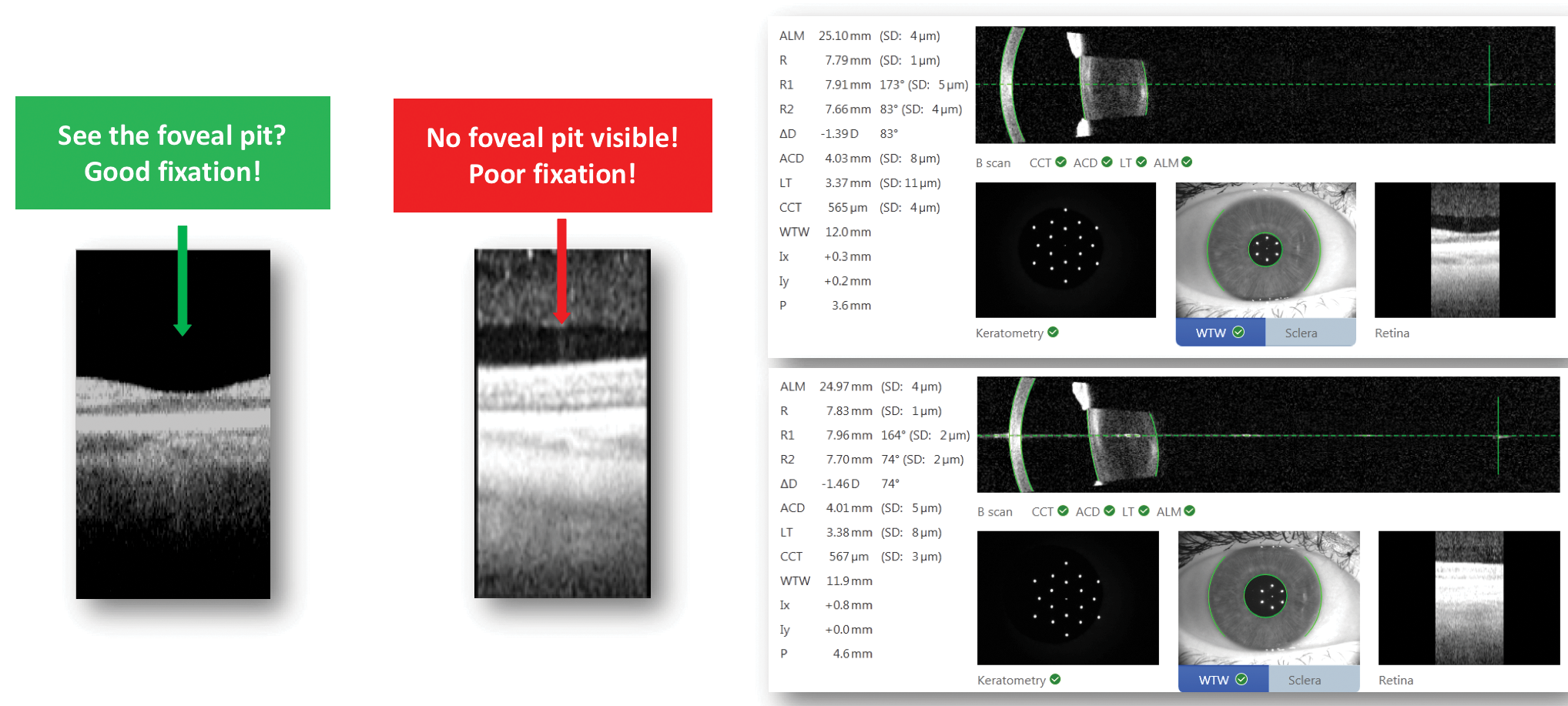
Figure 4. Advantages of swept-source OCT integration.
Image courtesy of Preeya K. Gupta, MD
Plus, it has unparalleled capability for data transfer. The ability to have biometry, IOL, and alignment data at your fingertips transferred to the surgical microscope is exceptionally valuable. It is more than just getting great outcomes; there is added value in helping to prevent errors.
Dr. Sadri: We have the IOL Master 700, and in fact we have 38 pieces of equipment from Zeiss in our practice. I think where the IOL Master 700 really comes into play is the objective refraction K and corneal K analyses. The big advantage, in our experience, has been the reduced need to perform the A scan. We don’t do these much anymore because the 700 has just such great optical clarity, both in the anterior and the posterior segments. I think that lends itself to a better outcome. We found that the IOL Master 700 picks up epiretinal membranes much faster, and I think that there are a lot of things that we still don’t know, in my opinion, about how effective this product is. But, I’m excited because the portfolio is very strong.
I believe that, if you are trying to get the best outcomes, OCT is mandatory in order to see to the back of the eye and eliminate any kind of surprise. I think evaluating the posterior segment has become essentially mandatory in my practice. It also allows me to have a really nice conversation with patients.
For example, I recently operated on a woman who came in for cataract surgery and was referred from an outside optometrist. We did a thorough analysis of her eyes and found a pretty large epiretinal membrane in her right eye, so we decided to put a monofocal IOL in that eye. Even though the cataract was dense and hard to pick up on an exam, the OCT really did a nice job of imaging the retinal tissue.
Dr. Solomon: Dr. Thompson, do you differentiate the preoperative testing you do in a routine patient versus a patient who wants a refractive outcome?
Dr. Thompson: Well, it almost becomes two exams. It used to be in a refractive evaluation, we would do the dominance test, followed by tear film testing, and then we’d do the topography. But in a cataract evaluation, we would do topography, biometry, and OCT. Now, with the availability of so many premium IOLs, when we know we may need to do a corneal refractive surgery touchup postoperatively, it’s like both a refractive corneal exam and a cataract exam all in one.
One of the things that I love about the IOL Master 700 technology is the accuracy of measurement, as well as other things that matter in a good refractive and cataract evaluation. But in addition to this, it also gives us a glimpse at things like the macula (Figure 5). That’s a nice screening tool because it can tell you whether or not you need to look at the macula more closely. But, I see it as a blending of what used to be two different exams.
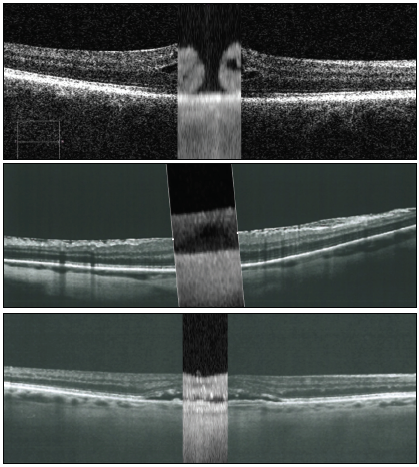
Figure 5. Finding macular pathologies with the IOL Master 700: macular hole (top), macular pucker (center), and age-related macular degeneration/retinal pigment epithelium detachment (bottom).
Images courtesy of Walter Sekundo, MD, PhD
STRATEGIES FOR THE PREOPERATIVE EXAM
Dr. Solomon: Dr. Yeu, do you differentiate patient exams depending on what they want to achieve postoperatively? If someone comes in and says, “I just want what insurance provides,” versus a patient who says, “I would love to be able to be less dependent on my glasses.”
Dr. Yeu: All of our patients get the same biometry and topography, but an OCT of the macula (OCTM) is not part of the standard protocol for every patient, and this is something that I hope to change. All of our patients interested in an advanced technology IOL, or those with diabetes or who have a known diagnosis of macular issues will get an OCTM. This is what I love in terms of the capability of the IOL Master 700; it is such a great screening tool. Those who we know are going down the route of wanting greater refractive freedom, of course, we’re doing a closer look at the macula. But we do not get a standard OCTM on every patient.
Dr. Solomon: Dr. Sadri, what do you do in terms of preoperative patient exams in those who want a more basic package versus those who want a high-precision refractive outcome and the chance for spectacle independence?
Dr. Sadri: I have been practicing long enough to know that the preoperative exam should be standardized, regardless of what kind of package the patient wants. The bottom line is that we are still ophthalmologists, and we have to provide comprehensive eye care to all of our patients. Let’s say a patient comes in and says, “I just want what my insurance covers,” we respect that, and we also understand that, at the end of the day, if you treat that patient well, his or her neighbor might eventually come in and you might get that business, and that business might be a premium IOL. A happy patient is a referring patient.
Dr. Solomon: Dr. Vukich, do you do anything different?
Dr. Vukich: Should a refractive surprise occur, we typically consider an enhancement on the cornea. Although it is uncommon, the ability to do so when necessary is important for patient counseling and for managing expectations.
Swept-source OCT on the IOL Master 700 allows us to image the macula and has enabled our technicians to confirm that they have a high-quality exam. We don’t do an OCT on every patient, but if the IOL Master 700 shows something that is atypical, then we use that as an indication for obtaining an OCT.
The ease with which my technicians can capture the data with the swept-source OCT has made it much easier for all of us. The IOL Master 700 will capture data even in eyes with very dense nuclei; it will capture eyes that we never could have captured before. It is now rare to have to do an immersion ultrasound.
Dr. Solomon: So, Dr. Thompson, you mentioned using multiple tests. So if my mom came to you and said, “Dr. Thompson, I want to see better, and I would prefer not to wear glasses.” What are you going to do in terms of workup for her?
Dr. Thompson: Well, I’m going to say, I consider it a great compliment to be seeing the mother of a very well-respected refractive cataract surgeon.
[Laughter]
Dr. Schallhorn: The pressure’s on.
Dr. Thompson: In all seriousness, we’d be doing our regular testing and that includes a refraction and topography. We’d be looking at her tear film very closely, her corneal health, and corneal multifocality. I want to know whether or not hers is a cornea that I can suggest something that is going to be scattering light, like an extended depth of focus (EDOF) or a multifocal lens. I really like to know how clean that cornea is before suggesting these types of IOLs.
Further, I’m going to be looking at her retina. If I find that her tear film is happy along with her cornea and her macula, I’m going to be talking with her about her preferences: Does she like the idea of doing a lot with glasses, or does she like the idea of doing a lot without glasses?
Dr. Solomon: She’s pretty demanding. She doesn’t want glasses.
Dr. Thompson: Then she’s going to want excellent vision at all three distances, and I am going to talk with her about monofocal monovision, EDOF, or low-add multifocal IOLs. I am also going to talk with her about mixing and matching to optimize functional vision at all three distances. I want to make sure she understands that this is oftentimes a two- or three-step process, per eye. When we do implants that provide good vision at all three distances, but the patient’s correction needs to be near 0, and if you have any healing issues that lead to residual refractive error, then we may need to do a laser fine-tune postoperatively, which I typically do about 3 months after cataract surgery. If there’s any haze in the capsule, we’ll need to do an Nd:YAG capsulotomy. I would tell your mom that after these advanced implants are in her eyes and after she has clear capsules (or had an Nd:YAG laser procedure), a happy tear film, and a happy retina, her chance for being very satisfied is extremely high.
Dr. Solomon: So, you talk about the possibilities of a laser enhancement with patients preoperatively as well?
Dr. Thompson: On every one of them. Because I tell patients that, even with traditional cataract surgery, the fine-tuner is glasses. With advanced cataract surgery, our fine-tuner is laser vision correction. And if you don’t need it, fine.
MEASUREMENTS YOU CAN TRUST
Dr. Solomon: Dr. Thompson mentioned topography. I’m assuming we all get topography on patients. So, what do we do when the topographical axis differs from our IOL Master axis, which might differ from our K axis, which might differ from our refraction?
Dr. Yeu: That’s where we pause and take a closer look at our measurements. But I think this goes back to the preoperative assessment. I always get a meibography on every single patient, simply because a lot of them are new to the practice, and it gives you a great snapshot in time of where their chronicity of potential ocular surface disease may be. Some of them truly have no discomfort at all, but you can see meibomian gland dropout and truncation, and you know that they’ve had some preexisting disease that, although it may not lead to staining, it could functionally affect the surgery itself and lead to greater symptomatic dry eye disease postoperatively. Doing a meibography alerts me to such potential problems.
With that being said, problems of the ocular surface are such a big reason for incongruity in K amongst devices, where staining from dry eye disease is the biggest cause, but it may be other causes, a mechanical epithelial basement membrane dystrophy, nodular degeneration, or dystrophic epithelium.
But the first thing we should be looking for is the why. The Placido-disc image is incredibly helpful to look at the quality of the corneal surface.
Dr. Solomon: But most of the time in normal corneas, I quite honestly find that the devices all vary because they all measure different parts of the cornea. So your magnitude and your axis is going to be a little bit different with each of these devices.
Dr. Yeu: There should be a certain agreement between devices.
Dr. Thompson: Well, when I have a device that measures total corneal power, I’m going to align based on that.
Dr. Yeu: Absolutely, I agree.
Dr. Thompson: And when I have a device that doesn’t measure total corneal power, I would align based on the anterior corneal curvature and know that I’m not doing it as well as I could. I’ll tell you something, I am very much looking forward to having a device that can do just that.
Dr. Solomon: Dr. Vukich, what do you think?
Dr. Vukich: The most common cause of atypical topographies is not forme fruste corneal disease or basement membrane dystrophy, it’s tear film disruption. If you get an abnormal topography, it is important to stop and ask yourself “Why is this the case?” You have to confirm that the tear film is adequate. If you choose not to use a toric lens because you were fooled by poor tear film quality, or if you choose a toric implant but place it in the wrong axis because you were fooled by the tear film, then you have not done your patient a service.
Dr. Solomon: Exactly.
Dr. Yeu: That’s right.
Dr. Sadri: There’s an art to medicine that I think we’re still learning. We’re working on it and we’re close, but we still have some way to go. I think the biggest thing is no matter how accurate you are or think you are with your measurements, you’re going to get some surprises postoperatively. There are a lot of patients out there with meibomian gland dysfunction, epithelial membrane disease, and epithelial dystrophy, for instance. I think it’s hard, and sometimes we miss the signs. At the end of the day, you have to be honest with the patient. You can do all the tests in the world and have the most fancy equipment, but you still have to deliver what the patient wants.
Dr. Solomon: So let’s return to Dr. Vukich. What’s your go-to device, if your topography is off by 5º from your IOL Master and your magnitude is off by 0.25 D?
Dr. Vukich: I tend to trust my instruments, but if there is a disparity, I go with the IOL Master 700. It provides the most consistent outcomes.
Dr. Yeu: I would agree because also, unlike Placido-disc topographers, which measure approximately the 3.2 mm zone, the IOL Master measures a much tighter zone within the central cornea. Thus, it gives me a closer average, and it also helps me to see what is going on power-wise through the visual axis.
Dr. Schallhorn: Another factor in favor of using data from the IOL Master 700, is that you can positively and quickly confirm fixation, an important component of ensuring good biometry data. I find that, if you observe varying K values, it’s generally either a dysfunctional tear film or poor fixation. With the IOL Master 700, you know that fixation is accurate.
THE ADVANTAGES OF VERACITY
Dr. Solomon: I think we’re all in agreement with using biometry, but I think it’s helpful to have other measurements as checks and balances. This helps us to ensure that the measurement we’re going with is likely correct. But it’s clear, if you’re looking at topography, optical biometry, OCT measurements, and refractions, it’s a lot of information to distill. Certainly, in today’s world and with the increasing usage of electronic health records [EHR], it’s almost impossible to find key information in the medical record, whether it’s pseudoexfoliation, an epiretinal membrane, or corneal basement membrane dystrophy, as you mentioned, Dr. Yeu. But we should be able to get at all of this discreet data from some of these devices. Dr. Yeu, what do you think? Is there a software solution that may help with that? Does that intimidate you? Does that excite you?
Dr. Yeu: It is exciting. This is an area that we can make the biggest changes as surgeons. From this point forward, it provides automated integration to not only make sure we’re doing all that we need to for insurance purposes but also to integrate everything very quickly and simultaneously. When we can see the information and get guidance on what lenses we should be considering based on this data, and then following that up with automated populated data of the patient’s postoperative outcomes, that’s not only extremely helpful, but it’s potentially game changing. This is where, in my opinion, Veracity (Carl Zeiss Meditec) is shining. (Editor’s note: For more on Veracity, see the sidebar below.)
VERACITY: INNOVATION DELIVERED
Veracity Surgical is a web-based software system designed by cataract surgeons to integrate with electronic health record (EHR) systems and diagnostic devices to help surgeons work faster and make better decisions for their patients.
Some of the features of Veracity include:
- IOP power selection;
- Toric IOL (Barrett and Abulafia-Koch) and arcuate incision calculators;
- Surgical scheduling;
- EMR interface and integration;
- Diagnostic device data integration; and
- Patient-centered and supported design.
Veracity Surgical is an intuitive tool with applications that can be used throughout the entire surgical cycle. It guides the surgeon and surgical staff in surgical planning and during the surgical procedure (Figure), assists with surgical scheduling, facilitates communication within the team, and automatically assesses postoperative data to assist with outcomes analysis.
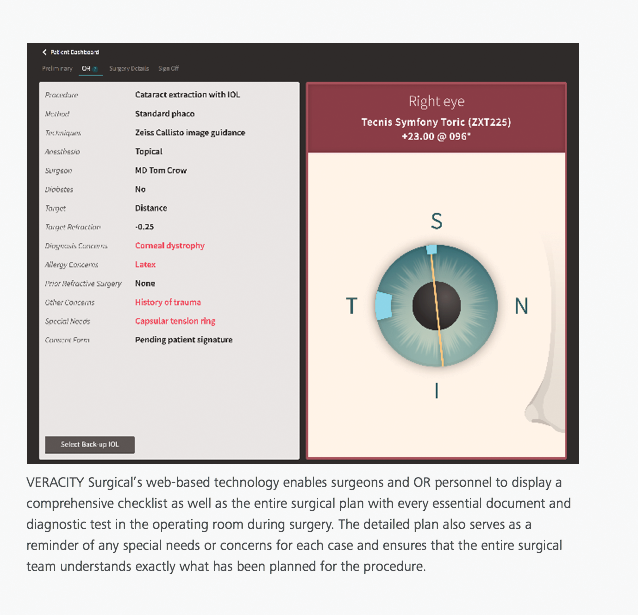
Figure. Example of a comprehensive checklist and surgical plan created by Veracity Surgical software.
Dr. Solomon: Let me talk a little bit about what Veracity is because not everyone is as familiar with this platform as you are. Veracity a new surgical solution designed to glean key information from the EHR, as well as key diagnostic information, and to help doctors make better surgical decisions in order for our patients to achieve better postoperative outcomes. Because it’s connected to the EHR, it should automatically pull the patient’s pre- and postoperative information, so that you can optimize your surgeon factors and your outcomes. Dr. Thompson, do you think something like that would be helpful?
Dr. Thompson: I think it makes EHR more relevant. It’s doing what you had always hoped EHR would do. I also think it helps surgeons better understand what their patients want. Veracity has this wonderful patient questionnaire that helps us as the surgeon understand the way the patient wants to use his or her vision postoperatively. In combination with the EHR, that questionnaire helps the surgeon to understand if there are any troublesome issues to be looking out for. Then all of the patient’s diagnostics can also be imported into Veracity for additional capability for accuracy.
Then, with one click, we can see the software’s recommendations for IOL power, astigmatism management, IOL selection. It generates documents for your chart and your referral letters. The ambulatory surgery center has the same data, so everyone is on the same page on surgery day. You are able to generate a referring doctor letter, and then—what we all want to do but struggle to find the time—this tracks our outcomes. And it absolutely amazes me how relevant Veracity makes the EHR.
Dr. Solomon: Many people confuse it with an EHR, but it’s not. The other thing is, it’s pretty efficient.
Dr. Thompson: Well, one click’s not too bad.
[Laughter.]
Dr. Sadri: I’m pretty excited about what the Veracity technology can do, which is to help provide automated and populated data in our machines. One of the things we tend to find with our technicians is that data entry from one machine to another is problematic. Veracity, I think, is a good solution that will allow a consistent stream of information flowing between the different platforms, most diagnostically in EHRs. That will save you time, which means more resources for the practice and, most beneficial, more time with the patient instead of away from the patient.
I think there’s an enormous amount of additional costs that comes in when the technologies used don’t talk to each other, and that cost is human time. Payroll time I call it, which basically eats into the growth of and the profitability of the practice. Anything that is going to help reduce that payroll time is important. I think that Veracity has shown a substantial ability to do just that.
Dr. Solomon: If you calculate the time it takes to plan surgery, a routine case, on average, it’s about 5 minutes to create a file folder and write your plans down and put all the supporting elements in a binder. But for a more involved surgery, say a toric lens or a presbyopia-correcting implant with or without astigmatism, it can be 15 to 20 minutes per eye to plan the surgery. Veracity does it in about 3 to 5 seconds. So, we do it in real time in front of the patient.
Dr. Thompson: So not only is it software, it’s smart software.
Dr. Solomon: It’s going to save practices time, and it’s going to save practices money. Dr. Vukich, would something like that be helpful in your practice?
Dr. Vukich: We use FORUM (Carl Zeiss Meditec) for data management, glaucoma evaluations, retinal evaluations, and image management. I believe FORUM is a great product, and I think Veracity is now the add-on technology that brings even greater functionality to the FORUM platform.
What appeals to me about Veracity is having a dashboard, which simplifies the ability to look at data from multiple devices. To have all of the relevant data in front of you as a preflight checklist is extremely beneficial. It minimizes the potential of making a mistake. The data are there, all packaged on Veracity, and they create another level of confirmation. This is yet another way to insure that you to provide the best possible care for your patient.
Dr. Schallhorn: As has been discussed, Veracity hits all the bases of what surgeons need to review before cataract surgery, and it does so quickly, efficiently, and with less chance of error. You know something is solid when you look back on it and say, this is obvious—why haven’t we been doing this before now? Why haven’t we had a system like this in the past? You know it’s right when you reach that point. And, I think Veracity is that point. The first time I saw it, I found myself asking why hasn’t this been done in the past? Veracity pulls together all the most important surgical information at our fingertips. I think that’s as good an indication as I can think of that this technology is relevant. We need this.
COMPLEMENTARY TECHNOLOGIES
Dr. Solomon: Let’s move on to the OR. You mentioned CALLISTO, Dr. Vukich. Tell us about what you like about CALLISTO and what you use it for.
Dr. Vukich: CALLISTO has made it easier for us to be consistent in several aspects of our IOL surgeries. First, with our capsulotomies, CALLISTO provides an image that works as a guide for a round and centered capsulorrhexis. I use a manual capsulotomy technique, and the CALLISTO has helped me become more consistent. It has a high-quality camera and a recording system. I record all of my cases. I have recorded them in the past, but CALLISTO facilitates that and makes it even easier to be able to capture still images at very high definition.
Second, CALLISTO accurately confirms the axis to place a toric implant. It provides a real-time, heads-up display through the microscope that shows exactly where the implant is to be positioned. After I’ve evacuated the viscoelastic at the end of the case, I turn the CALLISTO back on and check if any hydrodynamic torquing of the implant has occurred. I’m using CALLISTO in 100% of my cases, and I find it efficient and effective.
Dr. Solomon: It is such a robust tracker. I’ve used it, and I agree with Dr. Vukich. The tracking system on CALLISTO eye is phenomenal. I find that, with my instruments in the eye or out of the eye, that tracker is incredibly robust in sensing any movements of the eye. Compared to the way we used to mark an eye with a blue ink pen, how would you compare your experience using an image-guided system versus what we used to do?
Dr. Vukich: Before CALLISTO, we’d been using a ink-marking mechanism or method for quite a while. When we tested how CALLISTO eye compared with an ink-marking technique, we found it’s more consistent and more accurate. There’s no question about that. With manual marking, sometimes you don’t always touch the limbus exactly where you wanted to, or you’re not exactly at 180º. Axial alignment with a manual marking technique isn’t 100% perfect. With CALLISTO, we eliminate the potential for these errors.
ASSISTING IN THE INCREASED USE OF PREMIUM IOLS
Dr. Solomon: The penetration of toric and presbyopia-correcting implants continues to grow, but some people are hesitant to use them, or rather they may not be confident enough to use them regularly. Where do you think these newer innovations fit in—whether it be accurate biometry, software to help minimize errors, or intraoperative image guidance? Do you think that these innovations are going to help improve the confidence people have when using toric IOLs and other premium IOL technologies? Especially if we’re optimizing their surgeon factors and increasing the likelihood that they’re going to help patients achieve what they want. Is that possibly going to help increase penetration in the market?
Dr. Thompson: I think it will help a ton. What surgeons want to do is make their patients happy, and when you have software that helps to figure out what needs to be done to get the patient what he or she wants, it’s a win-win. The kind of system that Veracity is helps you, in smart ways, choose the right IOL technology by calling upon a database of results from very experienced surgeons around the world—you have multiple surgeons’ opinions with this smart software. It gives you increased confidence, and it also can help you to educate the patient properly, to do great biometry and accurate calculations that will in the future incorporate things like posterior corneal curvature, and to help ensure that premium lens technology is properly aligned. I think it will move the needle in surgeons wanting to deliver advanced technology to patients.
Dr. Schallhorn: Used collectively, these technologies can help surgeons more consistently achieve good outcomes. This is part of taking your practice to the next level, helping you to consistently have happy patients after surgery.
But let’s back up to some basics. We should help to educate the ophthalmic community on the patient-centric benefits of premium IOLs, such as toric lenses. There can be a significant quality-of-life value to our patients to correct their corneal astigmatism during a cataract procedure.
Dr. Solomon: Dr. Yeu, can you chime in here and give us your perspective on using the premium technologies we’ve been discussing?
Dr. Yeu: Sure. If you just dabble in refractive cataract surgery—say you’re doing just a handful of toric or presbyopia-correcting lenses a month—at that point, you can continue to rely on basic equipment and still have good outcomes. But simply adding an advanced biometer, like the IOL Master 700, will help that surgeon progress to excellent outcomes, even with that one additional technology alone.
But when you garner a higher volume of refractive cataract surgeries, you have a commitment to your practice and to your patients to tighten your refractive outcomes. In order to do this, in my opinion, it is advantageous to increase the number of advanced technologies you use. Just by having those advanced technologies at your fingertips, you will be able to better nail your refractive predictability for all of your patients, particularly in the nonaverage eyes, like those with extremes in axial lengths or post-LASIK corneas.
Another reason that having advanced technologies available to you is advantageous is that, as we move into the next decade, a lot of reimbursement models and alternative payer systems will be based more heavily on patient satisfaction. Keeping that in mind, we’re going to get closer and closer to achieving a high level of patient satisfaction by utilizing the technologies that allow us to get there. And you don’t have to have every piece, but if you have something like an IOL Master 700, which is so accurate in terms of K values and the biometry it provides, and you combine that with intraoperative guidance, that will give you the tools you need to get your lens aligned where it needs to be. With these things, you’re doing your due diligence to help get the patient in that sweet spot at the end of the day.
Dr. Solomon: Great answer, Dr. Yeu. Dr. Vukich, do you have anything to add?
Dr. Vukich: The patient experience starts the moment the patient meets you. We’re getting to a point now where it is not only an expectation that we can meet the refractive result, but that every step of the way, patients are comfortable with the decisions they’ve made, the choices that they’ve made, and how the plan was implemented.
What was their experience like in the OR? How smoothly did the surgery go? How long did the procedure take? Were the nurses nice to them? These are all things that I believe are within the scope of what a premium practice is all about. We as surgeons fixate on the end result—what was the quality of vision? Of course, that’s critical, but I think it’s also critical that patients understand how we got them to that point. That’s part of the patient experience as well.
TARGETING ASTIGMATISM CORRECTION
Dr. Solomon: I want to back up for just a second and talk a little more about astigmatism. Dr. Thompson, in your opinion, what is the best method to nail that accuracy with toric IOLs? How much astigmatism, Dr. Yeu, will you leave on the table when you’re treating with LASIK?
Dr. Yeu: I leave 0.25 D at most.
Dr. Solomon: Is that number different for anyone?
Dr. Thompson: Well, you dial in for 0—with LASIK, you go for it all. So you go for 100%.
Dr. Vukich: You attempt that, but commonly there will be some residual refractive error. I would then look at the patient-reported outcomes before deciding to do a touchup. So if they’re -0.25 or 0.50 D, 20/20+2, I don’t go back and try to treat that.
Dr. Thompson: Unless it’s symptomatic.
Dr. Solomon: But on the front end, which is where I’m getting at, we treat all astigmatism. I hear at meetings and in different places, a lot of our colleagues will say regarding astigmatism correction at the time of cataract surgery, “Anything under 1.00 D, I ignore.” If you look in the marketplace, it is quite clear to see that we have all these tools that can help us to treat much less than 1.00 D of astigmatism. Now, we’ve talked about K, and we’ve talked about intraoperative guidance, CALLISTO, and others. How often do we need these tools? Really, would 10% of our patients benefit from this technology? Would 30% of our patients? Dr. Vukich, what percentage of our patients, globally, would benefit by having their astigmatism corrected?
Dr. Vukich: What we’re doing now is prescribing an implant with the same level of accuracy as a pair of glasses. Rarely would I prescribe glasses and ignore the astigmatic component.
Dr. Solomon: OK, so forget cost for this scenario and tell me, Dr. Thompson, what percentage of patients who present to you should you be addressing their astigmatism? What percentage of patients would benefit from astigmatism correction?
Dr. Thompson: All of them—I would honestly say all of them. For me, the way I like to think about it, especially if someone wants to see without glasses, is that we’re going to be using an EDOF or multifocal lens, or in some folks monovision, but all three of those scatter light. And they do it in a way that we can still achieve very high patient satisfaction—as long as we can get rid of the other sources of light scatter, be it the tear film, the capsule, or residual astigmatism. We have to get rid of those sources of light scatter to allow this very sophisticated optic, with very scientifically based light scatter, to shine.
Dr. Yeu: You make a really good point. If I was to look at all of my cataract patients, it’s exceedingly uncommon that the patient has less than 0.25 D of corneal astigmatism. We really should be treating as little as 0.30 D of astigmatism, especially if it is ATR or oblique astigmatism. Ultimately, there are a few reasons that we need to treat even such a small amount of astigmatism. First, with any IOL, astigmatism will decrease contrast sensitivity. This is true to varying degrees, and moreso with diffractive optics, but they do affect the overall quality of vision. Second, eyes with -0.25 to -0.50 D of only residual sphere postoperatively will have better quality of vision ultimately than someone who you leave with a similar spherical equivalent, with a residual refractive astigmatic error.
Dr. Thompson: Right.
Dr. Yeu: Taking care of as much astigmatism as possible is ultimately going to help your outcome.
Dr. Solomon: If you look at data from Warren E. Hill, MD,2 among others, about 70% of our patients present with 0.50 D of astigmatism and around 85% to 90% of patients present with 0.25 D.3,4 The reality is that the vast majority of our patients who walk through our doors would benefit from astigmatism correction.
That just goes to show you how important it is to consider the use of toric IOLs, limbal relaxing incisions, and arcuate incisions—and this is true whether someone is doing monofocal lenses, presbyopia-correcting lenses, or other lens technologies.
Dr. Thompson: Even incision placement.
Dr. Schallhorn: I totally agree. This is the logic that ought to drive increased use of toric IOLs. In any large data analyses, they include patients with even 0.50 D of astigmatism. Even 0.25 D of residual or manifest astigmatism in a premium patient will, on average, slightly lower patient satisfaction. If we want to drive patient satisfaction up, we need to pay attention to this.
In my experience, all things being equal, more than 50% of patients would benefit from this. But I think it hasn’t caught on just yet, partly because of access to technology, but also because we need to be more confident in the accuracy of our measurements of the corneal power, confident in our ability to choose the proper lens, confident to implant it efficiently, and confident to align it properly. I think that technology is not yet there in the hands of many surgeons. It should be there, and we have it available.
EMBRACING NEW TECHNOLOGY
Dr. Solomon: On my OR day, my image-guidance system is on the whole day. It’s rare that I do a case without it these days because I’m doing some form of astigmatism management with whatever I do. Whether it’s with the femtosecond laser on the front end or a limbal relaxing incision enhancement or touchup on the back end, or a toric IOL, I’m managing astigmatism in almost every case. I agree, more surgeons need the tools necessary to get us all there.
Yet, oftentimes, there’s some hesitancy for people to integrate or adopt these technologies. Do we have any points or tips for surgeons? How do you adopt new technology? You guys all have it, but what about the practice that doesn’t? What advice or tips do you have for how to best implement or integrate this into their practices?
Dr. Thompson: First, I think one great option is to learn about it through a trusted colleague, and to prioritize learning about it. Put in the time. If you want to get into premium cataract surgery and get to the next level of accuracy, well, you need an advanced implant. And you want to make sure all of your measurements and your IOL power calculations are accurate. I would say quality biometry is at the top of that priority list. Second, you need to be able to align that IOL and to have a plan for in-surgery alignment. Third, ideally you would have something that helps you with patient education, and technologies like Veracity are wonderful. The companies are there to educate you on how to use it, but I think learning through a trusted colleague and educating yourself on these things are even better means to getting started. I found that, by handling my cataract surgery practice in a way that I give premium implants a platform, so patients can make a choice, it’s lifted the whole boat. It’s increased the traditional cataract surgery volumes also. The investment in time and money that I spent to incorporate these technologies was well worth it.
Dr. Vukich: It’s easy to say, “I’m a good surgeon and my patients are happy.” But what does that look like when you start collecting the data? How accurate are you for your attempted versus achieved refractions? Are you getting the sort of results that you believe are the best you can do? Improved technology will make all of us better surgeons. If we want to be a state-of-the-art practice, we have no choice but to use the best technology.
Dr. Solomon: Dr. Yeu, in your experience, is it possible that the staff could be resistant to change?
Dr. Yeu: That’s right.
Dr. Solomon: How do you deal with staff members who say something like, “The way we did it before was quicker and better.”
Dr. Yeu: Along the same lines, what about practices where each staff member serves multiple roles, where the front desk person checking in patients also doubles as the technician or the surgery scheduler? This happens a lot at smaller practices. Someone who is interested in moving his or her practice to the next level and is trying to get the practice to focus on patient outcomes must incorporate a refractive mindset for cataract surgery. The one thing that this person should be doing, if he or she is not already, as Dr. Vukich mentioned, is to utilize something like Veracity. That will actually decrease the amount of human resources needed to get to those pristine outcomes and to make the process easier for the surgeon, too. The surgeon also wears different hats, including doing IOL calculations; there isn’t enough time to also comb your own postoperative data to refine outcomes. That might not be the case in a larger practice, but it’s going to be the case in a smaller one. Something like Veracity is the perfect starting step to get the surgeon, with confidence, into a more accurate refractive mindset.
Dr. Sadri: The way that I see it, if you’re not growing, you are dying, and I think that most people understand that on some level. It’s true for large corporations, it’s true for large practices, and it’s even true for small practices. All of us, if we feel we’re growing steadily and getting better or evolving, then happiness will follow.
Going along with that is having the right staff, and that begins with the hiring process. Hire people with an innovative mindset, both physicians and staff. We routinely offer teaching and educational programs to our staff. For instance, we recently held a training on swept-source OCT on the IOL Master 700 OCT. You must do a good job of recruiting the right people and keeping them motivated. We are not perfect, we could always do a better job. I think that the practices that harness constant educational programs on the latest software or the latest hardware do a better job at retaining their employees and empowering them to be a part of the innovative mindset of the practice. I have found that the newer generation of technicians actually like technology, and they enjoy it, so we don’t find a huge barrier to adoption.
Dr. Schallhorn: I’d like to jump in here. I think that another barrier is that surgeons might shy away from toric IOLs because it is perceived as being difficult to successfully implant, whereas a monofocal IOL is easy. But these technologies make it much more straightforward and easy. It’s getting over that barrier, where realizing that putting in a toric IOL can be straightforward, it can be fast and efficient. That’s what we’ve been talking about—how to make it efficient and effective. Data captured with the IOL Master 700 are seamlessly transferred to CALLISTO in the surgical suite. You have Veracity to greatly aide in surgical planning. With one click in the OR, you’ve got the IOL power, and you can align the lens in the eye. These tools make it easy. So, we can overcome the barrier of, “It’s hard, it’s difficult, I don’t want to take that step.” Besides the other things we talked about, implanting any premium lens technology needs to be easy and efficient.
PUTTING IT ALL TOGETHER
Dr. Solomon: Dr. Schallhorn, that was great. Let’s go around one more time so that everyone can sum up his or her main points and a conclusion based on our discussion today. Dr. Yeu, would you like to start?
Dr. Yeu: We are in a really exciting stage with cataract surgery. We are finally at a point where we can integrate so many helpful technologies to simplify what has become an overwhelming process for not just standard but premium cataract surgery procedures. And so, with the technologies that are available to us, including software-integrating technologies—FORUM, for example—it is allowing surgeons to do what we’re supposed to do, and that is to be doctors and clinicians. Having technologies available that achieve a lot of the scut work and the legwork involved, it simplifies the process and gives us the algorithms and the tools necessary to make us better, more accurate doctors.
Dr. Thompson: I am amazed at how deeply incorporating premium technology and premium cataract surgery can energize a practice. Further, the effect it has on staff pride, on the confidence of our referring doctors, and on our community is invigorating. And so, I would say, adding these technologies is well worth the time and investment, and it really makes the practice of advanced cataract surgery very rewarding.
Dr. Sadri: We live in an exciting time, and there is growth in the marketplace in terms of the number of patients coming into our offices and in terms of those patients wanting the best technology. We’re very lucky to be in ophthalmology, as it is one of the few practices of medicine where we can innovate and provide good care, but also tap into the patients’ desire to want beyond what insurance typically pays. Companies like Zeiss are extremely important today because they really emphasize innovative technology platforms that we’re able to use in our suites and deliver what the patients want in a very elegant matter.
Dr. Vukich: The foundation of premium cataract surgery is doing a premium job for every single patient. That involves accurate biometry, accurate data management, and accurate execution in the operating suite. Implanting a monofocal lens with distance correction only requires the same level of expertise—the same level of careful planning and execution—as doing a multifocal or EDOF IOL.
Dr. Schallhorn: We can all agree that increasing clinical and OR efficiency, improving clinical outcomes, and making the surgical procedure more straightforward are all critical components to advancing your practice. The technologies we’ve been talking about during this roundtable are capable of driving every one of these important points.
Dr. Solomon: I agree. Essentially, what we’ve been talking about today is a refractive cataract suite, right? The solutions that Zeiss provides—biometry, data management, intraoperative alignment, and postoperative optimization—it is a complete solution to our needs as cataract surgeons. When I look at new technology, I look at it with two things. One, will it increase our outcomes? And to me, that’s not only getting the refractive outcome we’re looking for but avoiding errors. Two, is it going to make me more efficient? We all have seen the numbers, and we know that there will not be enough cataract surgeons in the near future to take care of the baby boomers. We’ve got to be more efficient with what we’re doing in order to treat these patients. Therefore, increased efficiencies will help us to save time and money in our offices and with our staff. If new technology can do that, then that’s a winner for me. I believe that the technology we have available today from Zeiss does just that, and I think you all agree. Thank you all for your time and your insights.
1. Koch DD, Ali SF, Weikert MP, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080-2087.
2. Advances in refractive/cataract surgery. http://rhodeisland.aoa.org/Documents/RI/Handouts/Adv%20in%20refractive%20and%20cat%20surgery.pdf. Accessed April 9, 2018.
3. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, et al. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70-75.
4. Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36(9):1479-1485.








