


Growth in a Family Business
Shelly Williamson Esnard, PA-C, and Blake K. Williamson, MD, MPH, MS


Our grandfather was in the business of eye care more than 70 years ago, and his four sons followed in his footsteps. Three of them are ophthalmologists, and one is a physician assistant working in ophthalmology. About 50 years ago, our father founded Williamson Eye Center. The center’s focus on patient care has led our clinicians over the years to pursue procedures outside the scope of general ophthalmology such as state-of-the-art vision correction surgery and ocular aesthetics.
Early in his practice, in the late 1990s, Baron Williamson, MD, became interested in facial/oculoplastics. His foray into ocular aesthetics at Williamson Eye Center was performing blepharoplasties, brow lifts, and CO2 laser resurfacing. Simultaneously, the first cosmetic indication for onabotulinumtoxinA (Botox Cosmetic, Allergan) was granted by the FDA for the treatment of glabellar lines. This was the spark that led us, in the early 2000s, to create an aesthetic arm to the company that focused on laser hair removal, skin care, collagen injections, laser tattoo removal, and the cosmetic use of Botox as an alternative to plastic surgery.
At that time, our aesthetic rooms were located at the back of Williamson Eye Center, close to the surgery center. When patients came in for a LASIK consultation, they were encouraged to meet with a cosmetic coordinator who championed our menu of elective procedures. The coordinators introduced them to LASIK, blepharoplasty, and nonsurgical options such as Botox Cosmetic. We had an aesthetician on-site to perform the nonsurgical procedures such as facials, laser hair removal, and microdermabrasion.
Having our aesthetics services located at the back of the eye center had its challenges. On the one hand, we could leverage the credentials and significant patient volume of the Williamson name in our community; on the other, we could not create a unique brand for these services or cater to that clientele. Ultimately, we outgrew the space we were in and looked to expand. Additionally, we quickly realized that, as much as patients loved the idea of alternatives to plastic surgery, they still wanted the option of undergoing surgical solutions such as a facelift, rhinoplasty, brow lift, breast augmentation, liposuction, and tummy tuck. In response, we partnered with a facial cosmetic surgeon, Jon D. Perenack, MD, DDS, in 2005. Some years later, we partnered with a body plastic surgeon, Lucius Doucet III, MD. Eventually, we spun off this part of the practice and moved it to a separate physical location, which helped distinguish our aesthetics brand from the eye center. Not long after, we rebranded our services as a separate practice, Williamson Cosmetic Center and Perenack Aesthetic Surgery.
SYNERGIES
The centers continue to collaborate. When cataract surgery patients comment that they notice their lines and wrinkles more often now that they can see better, our surgeons at Williamson Eye Center refer them to Williamson Cosmetic Center. Likewise, when cosmetic patients mention experiencing a decrease in their vision to one of our cosmetic providers, they are referred to Williamson Eye Center.
Practices that offer aesthetic medicine are expected to offer cosmeceutical skin care to patients to enhance their in-office results. Until now, a retail product option for patients undergoing eye procedures has not been available. Oxymetazoline hydrochloride ophthalmic solution 0.1% (Upneeq, RVL Pharmaceuticals) is the only FDA-approved prescription eye drop for acquired ptosis to lift the upper eyelids. State regulations determine the dispensary process (ie, dispensed directly to patients at the practice or by prescription). Offering this retail item to cataract surgery patients who elect a premium IOL and/or laser cataract surgery can often lead them to inquire about aesthetic services. Saying things like “Now that you can see beautifully, I want you to see how beautiful you are,” can make an impression on patients.
GETTING STARTED
The top two aesthetic offerings in the United States are currently neuromodulators (ie, neurotoxins) and dermal fillers (eg, hyaluronic acid). Offering these products is a great place to start in aesthetics for two main reasons. First, they require no inventory other than vials of the products and syringes. Second, the procedures can be performed by one person, whether an optometrist or an eye surgeon. As a result, the startup cost is low, and the return on investment is high.
Simply offering these procedures, however, is not enough to jumpstart aesthetic services in your practice. We recommend identifying one person to champion aesthetic services and train other staff members on how to talk to patients. It is also important to create solid standard operating procedures that include having a coordinator talk to patients about aesthetics. Interested individuals who are handed a brochure generally walk away. Those who talk to someone about pricing and scheduling options are more likely to book the procedure in our experience.
DIVERSIFICATION
From an economic standpoint, practices that do well with injectables may wish to expand their offerings into aesthetic surgery, laser treatments, and retail. (For more on retail, see “Selling Cash-Pay Health Products in the Office.”) Diversifying can help to balance the ebbs and flows often encountered in elective medicine. For example, when surgical volume is a little low, injectables and laser treatments can help support the practice.
Diversifying the practice’s offerings also creates a variety of touchpoints for patients throughout the year. Patients typically come back every 4 months for an injectable, and they may see their aesthetician six times a year. These individuals are embedded into the practice, and they feel like they are a part of your practice. This can help drive the surgical business because these patients entrust their care and the care of their family and friends to the practice.
Williamson Cosmetic Center is trending in the top 50 practices in the country, according to Allergan. We are in the top 0.1% of Botox providers in the nation. To share our knowledge, we created a training company, The Aesthetic Platform (TAP), that helps others set up a full aesthetic practice or an aesthetic arm. TAP provides on-demand virtual and on-site clinical training and operational development programs. We also host fundamental courses and didactic presentations on neurotoxins and hyaluronic acid fillers that instruct health care professionals on patient assessments and injection techniques. TAP courses are led by one of us (S.W.E) or by our other faculty (Dr. Perenack and Kristi Robert, PA-C).
CONCLUSION
Williamson Eye Center and Williamson Cosmetic Center & Perenack Aesthetic Surgery are two separate entities with a unified clinical mission. The synergy between our business models is that both offer procedures and technologies that are not covered by insurance but are considered to be the state of the art and can improve patients’ quality of life and lifestyle.
Six Questions to Ask Yourself Before Committing to Grow Your Practice
Lisa K. Feulner, MD, PhD

Before opening my practice 18 years ago, I worked in two different care settings. The first setting was a large and busy multispecialty practice, and the second was a small solo practice. From these unique experiences, I learned what kind of doctor I wanted to be, what I wanted my day to look like, and the kind of culture I wanted to create. What I didn’t learn were the nuances of business. I picked up a few pearls from my experiences in both practice settings that helped me on my journey to opening and growing my practice. Few ophthalmologists were given the knowledge during training to develop and execute a successful business plan. Making choices by trial and error without a business plan can have costly consequences. A sound business plan may not prevent you from making mistakes, but it can help minimize the financial impact of those mistakes.
TAKING CALCULATED RISKS
Growing your practice involves a calculated risk. When I opened my practice, I had one employee and shared office space with four optometrists who had a large vision, contact lens, and optical base but didn’t provide medical or surgical eye care. This space-sharing arrangement was beneficial to both practices, and they grew together. I took advantage of their young patient demographic and large contact lens patient base to grow a successful dry eye, refractive surgery, and aesthetic practice. Ten years ago, I bought the optometry practice and doubled the size of my already growing comprehensive eye care practice. I now have three doctors, 30 employees, and a productive optical, aesthetics, and med spa practice.
Growth is key goal for most businesses, but how do you know when to expand your business? This question can be especially challenging to answer for physicians considering the addition of noncovered services and products to their practice. Many surgeons who offer refractive surgery and refractive cataract surgery, myself included, experienced some initial discomfort speaking to patients about paying for services or products. With practice, however, it is normal to develop a confident and comfortable way of presenting these cash-pay options. Discussions about elective offerings can become quite routine.
SIX QUESTIONS
Before you jump into a business venture, answer the following six questions: Why, when, what, who, where, and how? This is important, especially when considering adding a product or service line in an area where you may not be an expert, such as adding an optical shop or offering aesthetic procedures.
Why? The why is the most important factor in your business plan. Ask yourself why you want to add new products or services. What triggered your thoughts of expansion? Your business vision statement can provide you with valuable insights into potential areas of expansion within your practice. In my case, I had taken out a small loan to open my practice, and I needed to generate cash flow while I waited for the practice to develop a steady income. My friend and colleague Sheri Rowen, MD, FACS, suggested that I begin to provide aesthetic procedures such as Botox and a skin care line in my office. Both are fairly low-cost, low-risk ways to initiate aesthetic services, offer self-pay options, learn the required skills, and make the necessary adjustments in the practice.
When? Before deciding to expand, make sure your business is positioned for growth. Acknowledge your business limitations and identify how they affect your growth strategies. Next, set a time frame to expand. This may depend on your budget, staffing, space, and training needs.
It’s crucial to identify and develop one target market before introducing the next one. Often, the staff needs time to learn and incorporate new processes into the practice. Staff buy-in is crucial, and employees must be knowledgeable and comfortable each step of the way. Schedules and office space utilization may change, and providers may need to master new skills. This can take time.
Set a goal for adding a service or product and set financial and logistical milestones to achieve this. In my practice, we revisit our service offerings once every 6 months. For every service we add, I obtain training to evaluate patients properly, recommend products appropriately, and treat patients efficiently. The stimulus for the direction of growth must come from patients. Once I started offering skin care and Botox, patients began to ask for more products and services. At first, I provided aesthetic services within my existing exam lanes and treatment rooms. I added more doctors and staff as the demands for both the eye care and aesthetic services outgrew my ability to manage it alone. Eventually, I separated our aesthetic services from the eye care part of the practice. Both services are still located in the same building, but the aesthetic and med spa services share a separate entrance, staff, and treatment area.
If you’re not sure if it’s a good time or whether you’re financially prepared for expansion, seek advice from an expert who can provide a comprehensive expansion strategy. This can save you time, money, and costly mistakes.
What? Determine what products and services your patients may want. When I started my practice, I was one of the only providers in my community offering aesthetic procedures, and the demand for and interest in more services was compelling. I gradually added dermal fillers, intense pulsed light, laser hair removal, laser skin rejuvenation and wrinkle reduction, noninvasive fat removal, and aesthetician services such as facials and chemical skin peels. Additionally, I started performing upper and lower eyelid blepharoplasty to complement my aesthetic offerings. (For more on blepharoplasty, see “Ready to Add Upper Blepharoplasty to Your Offerings?")
Laser hair removal, laser skin rejuvenation, and noninvasive fat removal can be financially rewarding. Adding the devices required of these procedures, however, requires a large capital investment. Careful planning is essential.
It was frowned upon to have an optical shop to provide vision exams and dispense contact lenses when I started in ophthalmology, and in many areas it still is. Referring optometrists were concerned that they would lose their patients if they referred them to practices that provided these services. Good communication with referring ODs and a strict policy never to provide a prescription and to return all referred patients to their optometrists can prevent hard feelings and the loss of referrals. With these guidelines in place, it is possible to incorporate an optical shop into your practice successfully.
A knowledgeable staff is essential to the success of any retail endeavor. I inherited the optical staff from the practice I purchased, and I learned about vision insurance and the retail side of optical from them. Absorbing this information can be challenging, and the availability of online options and large commercial stores that can sell products for significantly less than a small retail shop complicate the process. Patients, however, love to get all their care in one place with high-quality products, people they trust, and great customer service.
Where? Establishing where you want to expand your business (eg, optical or aesthetic services) can mean either a new location or adapting space within your existing office. Opening an optical shop in an existing office, for example, requires a significant amount of space. It can be a complex and expensive endeavor unless there is already room for modification and expansion. If you’re moving into a new space, the ideal location for the optical shop is at the front of the office near the reception area and waiting room (Figure 1). Aesthetics, on the other hand, can be performed almost anywhere. Ideally, the treatment area provides privacy and therefore should be located away from the main flow of the office (Figure 2). Starting with an exam lane until the clientele grows is sufficient.

Figure 1. The optical area of Dr. Feulner’s practice is located at the front of the practice.

Figure 2. The aesthetic waiting area (A) and treatment room (B).
As the services and patient base grow, the demand for more dedicated space will increase, and renovations may be required. A private entrance and waiting room connected to the main office allows ease of access and visibility between both areas (Figure 3). Separating the aesthetic division from the eye clinic emphasizes more of a spa-like environment and has a less clinical feel. In this setup, however, the loss of foot traffic and cross-referrals can limit exposure and make marketing more challenging and expensive.

Figure 3. The entrance to the aesthetic services center in Dr. Feulner’s practice.
Figures 1–3 courtesy of Lisa K. Feulner, MD, PhD
How? The last part of the puzzle is to figure out how to implement your plan. Do you have existing employees whom you can train in the new offering? Do you need to hire employees or providers? Do you have to take out a loan, or can you buy an existing practice? Acquiring another business is costly, but it can be the fastest route to growth and expansion. Merging with or acquiring another business can double the size of your practice, increasing potential sales and revenue exponentially.
Another part of the how is determining your potential net revenue and establishing a budget. What is the real cost of adding a service? This includes hard costs, disposable costs, space, time, and staffing. As you get ready to expand into a new market, determine the funds or resources you can allocate to the expansion. Doing so can help you determine what you can afford to do now and what you need to plan for financially in the future.
Focus on customer demands for products and services and the cost to purchase, provide, and sell them. Identify potential existing patients who might be interested in these services and focus your sales and marketing efforts on them. Target existing untapped interest within the practice. For example, if you do oculoplastic procedures or refractive surgery, ask those patients about their level of interest.
THE POWER OF SOCIAL MEDIA
After the organic growth strategy is implemented and successful, expand marketing avenues to include social media, print, networking, and community outreach. Social media is a powerful tool to promote your business to potential customers. Share before-and-after photos, create interactive content, and post videos often.
Take the time to build your networks. Networking allows you to cultivate relationships with other businesses and encourages them to refer patients to you through word of mouth. Hosting events is a great way to get to know your customers, educate them, and build relationships with them. Encourage existing patients to recommend your services, show appreciation for those referrals, and build brand awareness in the community by becoming involved in community events.
CONCLUSION
Offering noncovered services can be beneficial for your patients, exciting for the practice, and financially rewarding. Growing your practice requires determination, creativity, and good business practices and growth strategies. Regularly reevaluating your successes, challenges, and mistakes will guide future growth and expansion.
Adding Oculoplastics and Dermatology
William J. Lahners, MD, FACS; John P. Fezza, MD; and Joshua M. Newman, MD



One advantage of a private ophthalmology practice model is the ability to add retail and noncovered items and services. Retail items range from glasses and contact lenses to premium IOLs. Noncovered services can include diagnostics and treatment options for dry eye disease, elective refractive surgery procedures, and laser cataract surgery. Two revenue streams that are added less frequently are cosmetic facial surgery and dermatology. We added both to Center for Sight by recruiting an oculoplastic surgeon 24 years ago and a dermatologist 18 years ago.
CONSIDERATIONS
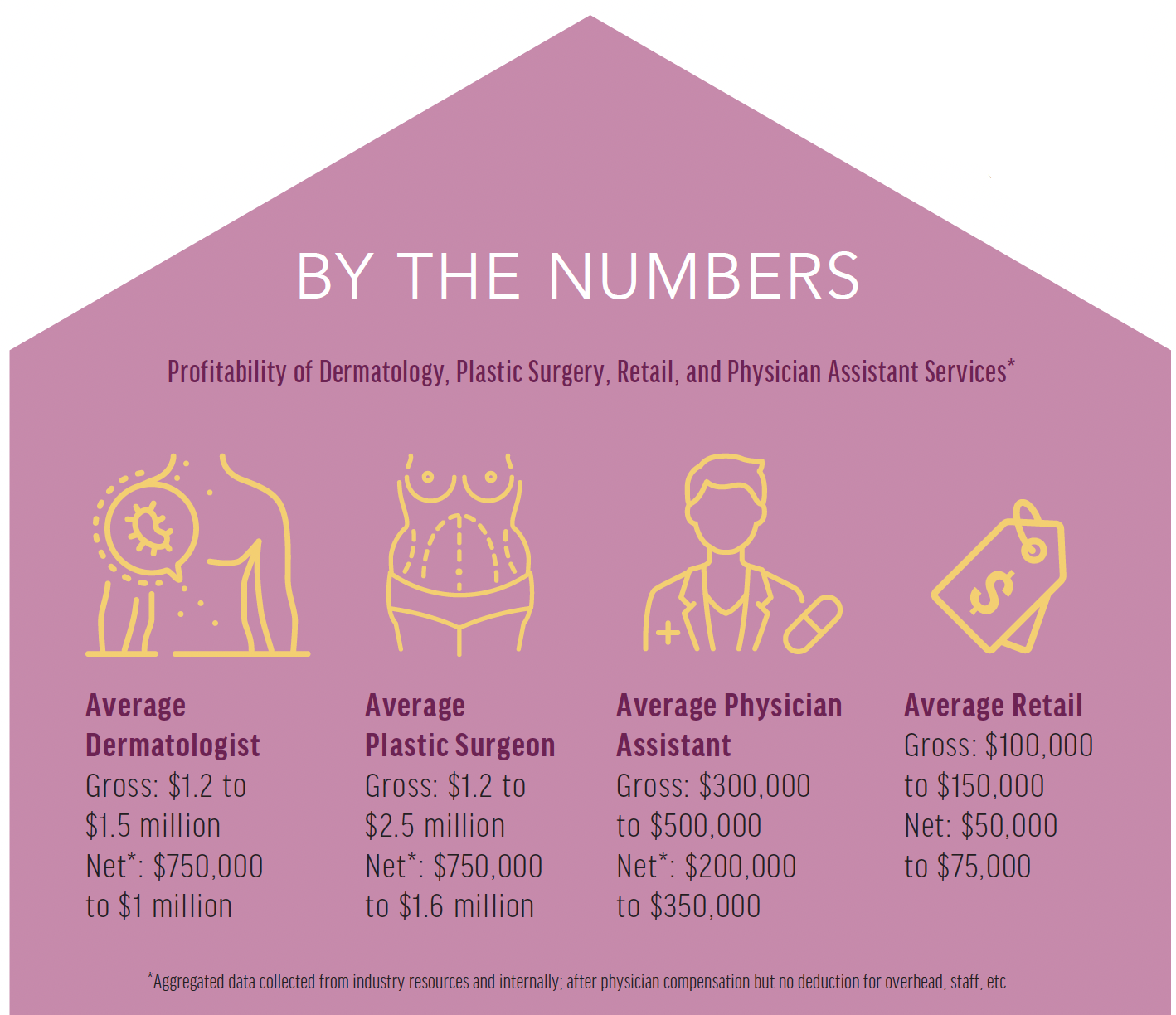
Plastic surgery and cosmetic dermatology involve an array of treatments that are not covered by insurance, and these can increase the profitability of an ophthalmology practice. Various cosmetics and products can be sold, and the revenue generated can be substantial (see By the Numbers). Little prep time (eg, no pupillary dilation) and no prephysician testing are required for these services. Less office space is therefore required for these patient consultations than for ophthalmic visits. For example, seven full exam lanes and a large room full of testing equipment are used for our cataract clinic. In contrast, oculoplastic consultations here use the equivalent of two or three exam lanes, and dermatological appointments use two or three exam/treatment rooms. Many of the procedures by each specialist are performed in a minor procedure room instead of a main OR, which helps keep our ambulatory surgery center profitable and minimizes competition for block time.
The big draw to cosmetic facial surgery and dermatology for us, however, was the overlap between these specialties and ophthalmology. Many of our premium IOL patients request referrals for cosmetic facial surgery or dermatology services. There are plenty of plastic surgeons and dermatologists in the surrounding area of our practice, but an extended waiting period is typically required to see the top providers. When a worrisome lesion was observed on a patient’s face before cataract surgery, these wait times could delay the cataract procedure. Having these providers in house allows us to fast-track consultations and treatment when necessary, and our patients appreciate the communication between specialists. This team approach is one of the most popular aspects of our multispecialty clinic.
DERMATOLOGY
Nationwide, the average wait times for a new patient appointment and a follow-up visit are 32 days and 6 weeks, respectively.1 At least 70% of the US population is considered underserved by dermatology. These problems are expected to worsen owing to the aging population, undersupply of dermatologists, and rising incidence of skin disease. When we added dermatology to our practice, our dermatologist’s schedule filled almost immediately with little promotion.
The profitability of dermatology is evidenced by the high rates of investment in the field by private equity firms.2 Dermatology can be procedure-oriented. This includes a high volume of biopsies and skin cancer procedures, which can provide a strong revenue stream (see By the Numbers). Dermatology also lends itself to leveraging the inclusion and expertise of midlevel providers such as nurse practitioners and physician assistants, which can add another layer of profitability to the practice (see By the Numbers). The vertical integration in this practice model can enhance the doctor’s schedule similarly to the synergy of optometric integration into an ophthalmology practice.
The focus on skin cancer in dermatology makes this specialty a natural fit for a cataract surgery practice. A major risk factor for the development of both skin cancer and age-related cataracts is UV radiation from the sun. Recent studies found that cataract patients develop melanoma and nonmelanoma skin cancer and precancerous skin conditions more frequently than patients without a diagnosis of cataract. Moreover, both skin cancer and age-related cataracts have been linked to a defect in the EPAH2 gene.3
OCULOPLASTICS
Many ophthalmology patients are interested in aesthetic procedures. After these individuals undergo lens-based or laser vision correction, they often become more aware of the effects of aging such as fine lines, wrinkles, and facial laxity. Much of their concern may focus on the area around the eyes.
When patients express concern to their eye care provider about these cosmetic changes, it is an opportunity for us to mention options such as blepharoplasty and to offer a referral to our oculoplastic surgeon. Our emphasis is on education, not sales. Our plastic surgeon may offer dermal fillers, neuromodulators, and complementary surgical procedures such as a brow lift, facelift, neck lift, or laser skin resurfacing depending on a patient’s needs and level of interest. Additional offerings include laser hair removal, vein removal, hair transplantation, nonsurgical fat removal, and intense pulsed light skin rejuvenation.
CONCLUSION
The addition of oculoplastics and dermatology has provided our practice with additional streams of revenue that are more resistant than ophthalmology to cuts from Medicare and private insurers. These parts of our practice became so popular and profitable that they were spun off into a separate entity—Amara Aesthetic Surgery and Dermatology—and moved into a free-standing facility next door (Figure 4). More importantly, our patients appreciate convenient access to multiple specialties and quality care.

Figure 4. The interior space of Amara Aesthetic Surgery and Dermatology, located next door to Center for Sight.
Courtesy of William J. Lahners, MD, FACS
1. Franki R. Wait times for dermatologist visits up 3.5 days since 2014. MDEdge. April 6, 2017. Accessed October 14, 2021. https://www.mdedge.com/dermatology/article/135218/practice-management/wait-times-dermatologist-visits-35-days-2014
2. Court E. Medical practices have become a hot investment—are profits being put ahead of patients? MarketWatch. June 19, 2018. Accessed October 14, 2021. https://www.marketwatch.com/story/doctors-are-being-bought-up-by-private-equity-and-its-your-health-on-the-line-2018-06-08
3. Sharma S, Lang C, Khadka J, Inacio MC. Association of age-related cataract with skin cancer in an Australian population. Invest Ophthalmol Vis Sci. 2020;61(5):48.

