You perform flawless cataract surgery on both eyes of a 68-year-old woman and you achieve 20/20 visual acuity in both eyes. At her 3-month postoperative follow-up visit, however, the patient reports vague discomfort in her right eye, which she insists began only after cataract surgery. No obvious abnormal findings are detected during a careful examination of the ocular surface. Tear osmolarity, meibography, and matrix metallopeptidase-9 findings are normal.
Nonetheless, you decide to initiate a dry eye and blepharitis regimen. To your dismay, no improvement occurs. Your patient becomes increasingly frustrated and expresses regret that she ever had cataract surgery. Because the eye looks normal, you begin to wonder if she would benefit from a consultation with a psychiatrist.

If you’ve experienced a situation similar to that described above, you’re not alone. If you haven’t, most likely you will at some point in your career. This patient had a particular type of recurrent corneal erosion that can be difficult to diagnose because there are no obvious corneal findings. These hard-to-detect recurrent corneal erosions are often overlooked and misdiagnosed. We ophthalmologists are trained to diagnose recurrent corneal erosions by eliciting a history of ocular trauma, inspecting the cornea for epithelial basement membrane dystrophy, and instilling vital dyes such as fluorescein to detect signs of epithelial irregularity or negative staining. In my experience, however, these standard methods are not foolproof. The use of a dry Weck-Cel sponge (Beaver-Visitec International) on the cornea has been described,1 but it is used rarely because of the risk of causing a corneal abrasion.
ADDRESSING A DIAGNOSTIC DILEMMA
There is a gap in our diagnostic toolkit for corneal erosions. In response, I developed a technique called the corneal sweep test.2 I developed this technique in 2017 and originally used a corneal spud to sweep the corneal surface to localize the erosion. This was quite effective—and I never damaged the cornea—but I was concerned that, if used improperly, the sharp edges of the tool could damage the corneal epithelium.
As a result, I developed the Kim Corneal Sweeper with Katena Products. This straight, handheld instrument with a smooth, rounded tip and a thin profile is designed for the corneal sweep test. In a 2-year retrospective study, this instrument allowed the clinician to survey the corneal surface in a safe and atraumatic way while detecting areas of loose epithelium easily (see How to Perform the Corneal Sweep Test).3
HOW TO PERFORM THE CORNEAL SWEEP TEST
Topical anesthetic eye drops are instilled with fluorescein dye. A lid speculum should not be used because blinking helps to moisten and coat the corneal surface evenly with the dye. The dye helps to highlight the loose epithelium when the cornea is swept. Under the slit lamp and cobalt blue light, the sweeper is placed on the cornea in a tangential manner and gently swept across the surface with slight indentation pressure to cause striae. The thin profile of the tip allows the clinician to visualize the cornea directly as it is indented (Figure 1). The instrument sweeps across normal corneal epithelium smoothly and atraumatically (Figure 2). If an erosion is present, the sweeper causes loose epithelium to move, resulting in a visible wrinkle (Figure 3). In my experience, these areas of loose epithelium tend to be discrete and well-demarcated. The sweeping maneuver does not cause the loose epithelium to spread into the adjacent normal corneal epithelium.
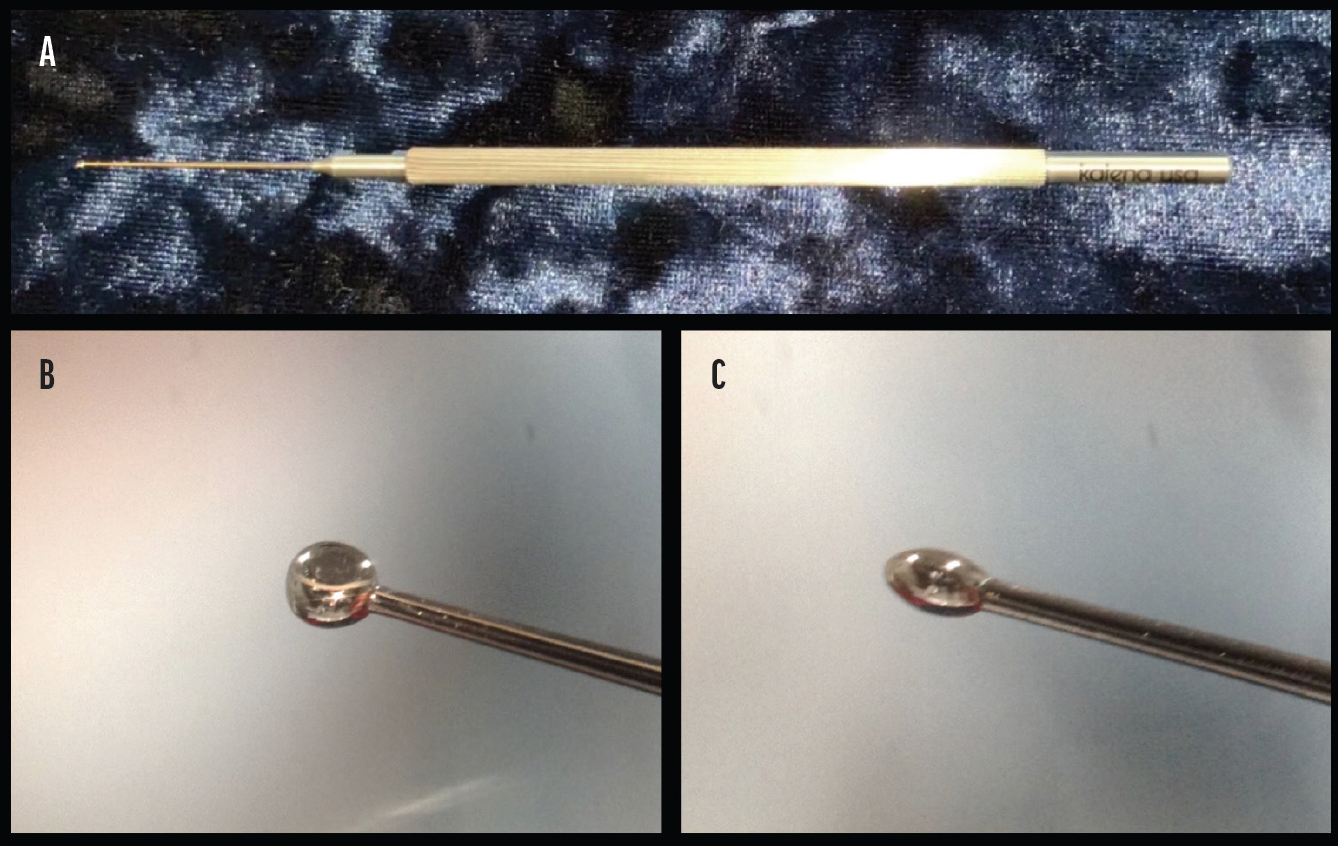
Figure 1. The Kim Corneal Sweeper (A). Front profile of the instrument showing its circular shape and smooth, round tip (B). Side profile showing its flat shape and smooth, round tip (C).
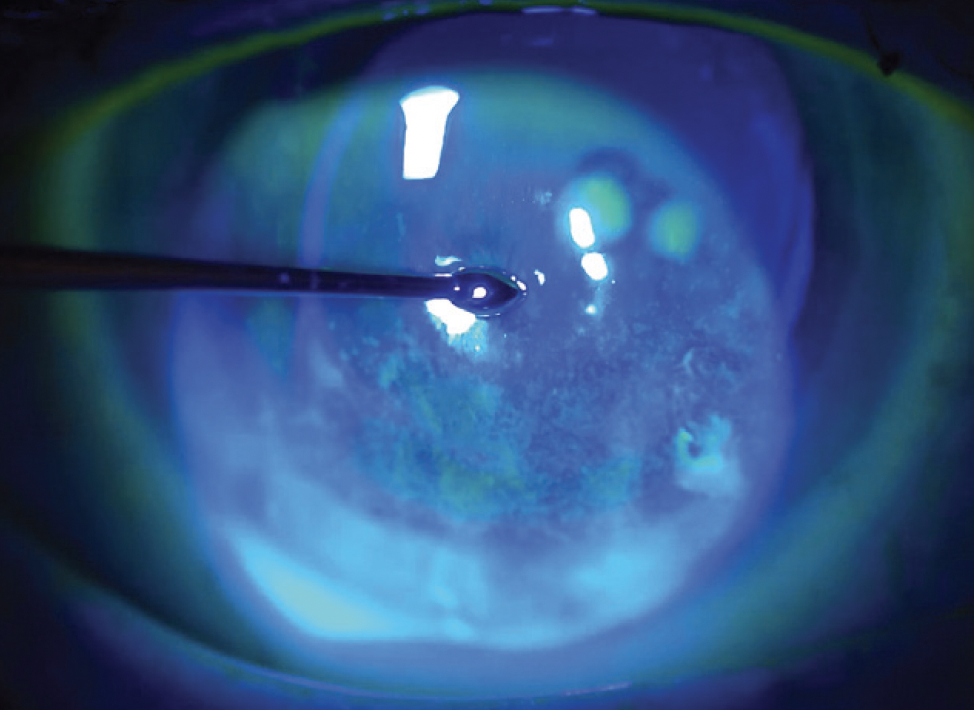
Figure 2. Fluorescein dye is instilled to stain the ocular surface, and cobalt blue light is used. The corneal surface is indented with gentle pressure; the maneuver causes no trauma to normal epithelium.
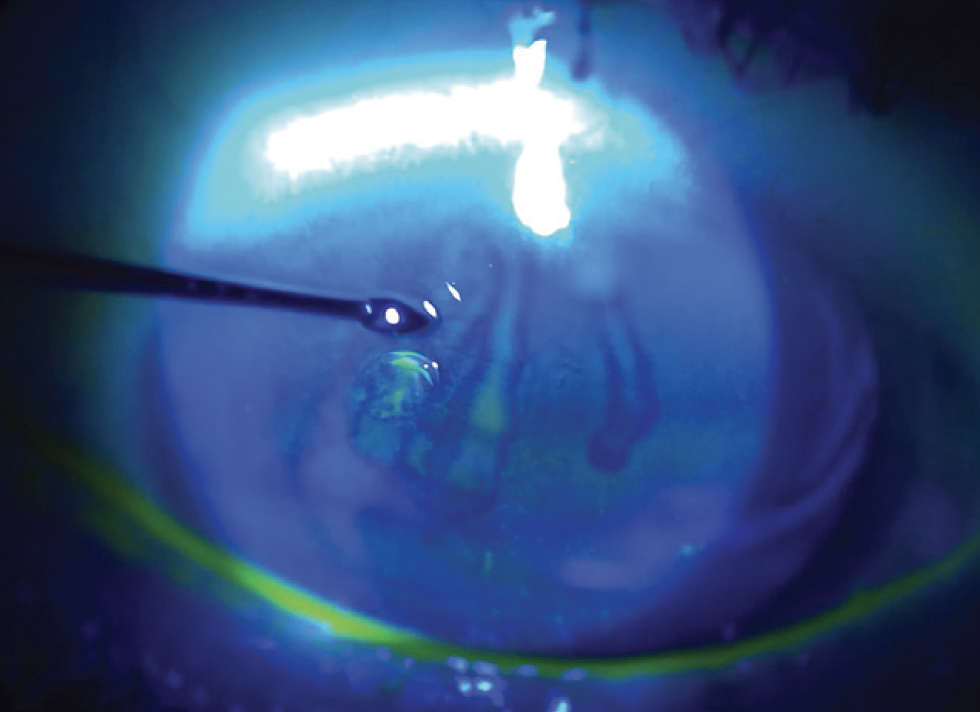
Figure 3. The corneal surface is indented with gentle pressure over the erosion, which causes the loose epithelium to move and creates a visible fold.
CAN CATARACT SURGERY CAUSE EROSIONS?
Ocular surface disease, epithelial basement membrane dystrophy, diabetes, and other risk factors can lead to recurrent corneal erosion. It is not, however, always a 1:1 correlation. Recurrent corneal erosions are a poorly understood, complex, and multifactorial disease process. Causation is difficult to prove.
Cataract surgery might not cause recurrent corneal erosion per se, but I believe clear corneal cataract surgery is a risk factor for this condition. The incision violates the epithelium, which can cause traumatic separation and poor re-adhesion of the epithelium to the underlying basement membrane.
RETROSPECTIVE REVIEW
My colleagues and I performed a 2-year retrospective chart review of 58 eyes with recurrent erosions treated in my practice.3 Of these, 34 had a normal-appearing cornea on slit-lamp examination but were diagnosed with recurrent corneal erosions after the corneal sweep test was performed and an area of loose epithelium was identified.
Clear corneal cataract surgery was the most common presumed mechanism of injury (28 eyes, 48.2%), and symptoms developed only after cataract surgery in 20 eyes (71.4%). All 20 of these eyes had an erosion located directly over the clear corneal incision. Most of our patients who developed symptoms after cataract surgery complained of pain and foreign body sensation. A small number had nonspecific and vague symptoms.
In our experience, postcataract surgery patients with persistent ocular pain syndrome often have an area of loose epithelium located over the clear corneal incision.2,3 I therefore believe that cataract surgery may be an important risk factor for recurrent corneal erosion syndrome. Whenever a patient says, “I never had this problem until I had the surgery,” clinicians should have a high index of suspicion for a corneal erosion. I’ve even discovered erosions in the eyes of patients who underwent cataract surgery many years prior. These patients can be treated successfully with hypertonic saline, a bandage contact lens, superficial keratectomy, or anterior stromal micropuncture.
CONCLUSION
A paradigm shift in the way we view recurrent corneal erosions is needed. This is not just a disease of accidental trauma but also a disease that can develop after cataract and corneal surgery. Approximately 10 million cataract surgeries are performed worldwide each year. Many of these patients are at risk for developing a persistent ocular pain syndrome from their clear corneal cataract incision. Further studies are needed to better understand this disease process.
I have found the corneal sweep test to be an effective and simple way to diagnose recurrent erosions and resolve patients’ symptoms. This technique could alter the way we approach recurrent corneal erosions and enable doctors to more effectively treat patients with persistent ocular pain.
1. Diez-Feijóo E, Grau AE, Abusleme EI, Durán JA. Clinical presentation and causes of recurrent corneal erosion syndrome: review of 100 patients. Cornea. 2014;33(6):571-575.
2. Kim ME, Kim DB. Cataract incision-related corneal erosion: recurrent corneal erosion because of clear corneal cataract surgery. J Cataract Refract Surg. 2020;46(10):1436-1440.
3. Kim ME, Kim DB. Implementation of the corneal sweep test in the diagnosis of recurrent corneal erosion: a two year retrospective study. Cornea. (Accepted for publication.)