

sponsored by




In today’s cataract market, the desire for great postoperative outcomes has added new meaning to IOL selection. Understanding how a patient plans to use his or her vision is an important factor to consider, especially when it comes to options for presbyopia correction at the time of cataract surgery. Because most patients want to return to an active lifestyle after their operation, providing them the vision that will allow them to do so means implementing a surgical plan that will improve both the quantity and quality of their vision.
With the wide array of IOL options available on the market, the ability to provide a patient the postoperative vision he or she desires has never been better. Key to designing an appropriate surgical plan, though, is gaining an understanding of his or her activities and lifestyle—and, in turn, how the patient plans to use his or her vision for daily activities.
The lens selection process typically involves a great deal of compromise: some implants are designed to provide distance vision, for instance, perhaps while sacrificing some ability to accommodate to near tasks. Other lenses are built to provide near vision that may entail some loss of the ability to see at distance. Meanwhile, monofocal lenses remain the most tried-and-true method for providing good vision at a fixed distance, even if they do not always provide vision at all ranges of distance.
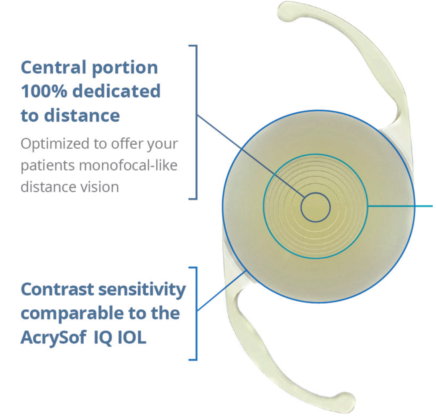
Newer advances in IOLs, however, may offer to change that paradigm. The addition of the ACTIVEFOCUS optical design makes AcrySof IQ ReSTOR +2.5 essentially a “hybrid” between a monofocal (distance) IOL, and a multifocal/presbyopia-correcting IOL (extended range). It has been specifically designed to address patient demand for a lens that provides the range of vision possible with a multifocal with the high-quality, uncompromised distance vision of a monofocal lens (Figure 1).1-3
Click here for Important Product Information
The Best of Both Worlds
The ACTIVEFOCUS optic contains a seven-step apodized diffractive area, with a central portion 100% dedicated to distance vision, added onto the AcrySof IQ IOL platform. The apodization is intended to yield highly efficient light management, such that more overall light is allocated to distance focal points at any pupil size.
AcrySof IQ ReSTOR +2.5 D IOL Directions for Use; Alcon Data on File (11 Apr 2016).
Figure 1. Model of AcrySof IQ ReSTOR +2.5 multifocal IOL showing the ACTIVEFOCUS optical design.3
In turn, the consideration for light management has important implications for visual performance, including helping to decrease the potential for visual disturbances.
Where the ReSTOR +2.5 IOL with ACTIVEFOCUS optical design differentiates from others on the market, however, is that its central portion is 100% dedicated to distance vision.
The result of this engineering consideration is a more even distribution of light across concentric radii around the center of the pupil compared with other presbyopia-correcting IOLs (Figure 2).4 In practical terms, this functionality answers a prevalent concern among cataract surgeons: In a recent survey of 90 surgeons, they said that the ability of a presbyopia-correcting lens to provide optimized distance vision was one of the most important vision attributes to address.5
While these features are important, they do not interfere with the performance metrics that surgeons have come to rely on with the AcrySof IQ family of lenses. The unique distance-dominant ACTIVEFOCUS optical design was added to the AcrySof IQ platform, using the same spherical aberration correction factor to achieve comparable contrast sensitivity to the IQ monofocal.3,6 Moreover, the aspheric construction improves image quality for distance vision under mesopic conditions.2 In all, the ReSTOR +2.5 IOL with ACTIVEFOCUS optic is designed to offer patients the best of both worlds: a blend of quality distance and an extended range of vision, with the potential for fewer visual disturbances.3,4
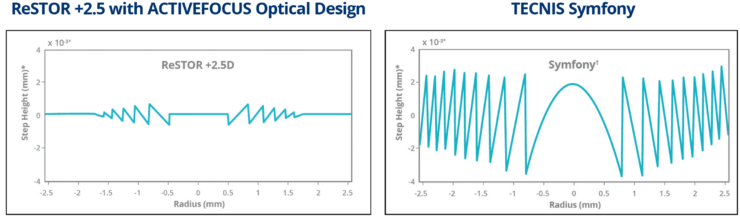
*Scaled to mm from microns (μ) for readability.
†Surface profile of the TECNIS® Symfony 28.0 D IOL was measured using Bruker Contour white light interferometer on the posterior surface and the diffraction efficiency calculated. Optical profile of the ReSTOR +2.5 D, model
SV25T0 is based on its design profile.
Alcon Data on File (11 Apr 2016). Alcon Data on File (06 Oct 2016).
Figure 2. Optical profiles for AcrySof IQ ReSTOR +2.5 IOL with ACTIVEFOCUS optical design and Tecnis Symfony Extended Range of Vision IOL.*
Click here for Important Product Information
Options for Refining Postoperative Vision
In the past, achieving an extended range of vision after cataract surgery and IOL implantation may have required a mix-and-match strategy, either by using a blend of lens options or by targeting different refractive goals in each eye. Such an approach would typically require a compromise in one or both eyes in terms of the facility to see at a given distance. It also potentially required the patient to neuroadapt to different visual stimuli in each eye.
Yet, while the ReSTOR +2.5 IOL with ACTIVEFOCUS optic is designed to give patients uncompromised distance vision with an extended range of vision, some patients may want their postoperative vision more finely tuned to one particular zone. For instance, individuals with hobbies and activities that require excellent near vision—such as reading, painting, looking at a smartphone, and playing sports—may want an additional near add in their fellow eye. For these patients, choosing a different lens for the second eye surgery may help them achieve the outcome they want.
Whether patients will want a blend of lens options is highly individualized and the timing of when to use each option will likely be dictated by situational need.
In either case, a clinical study and experiences in our own practices indicate that it is possible to successfully “blend” two multifocal IOLs—ReSTOR +2.5 with ACTIVEFOCUS optical design with ReSTOR +3.0—and potentially yield up to 2 extra lines of functional near vision, all without compromising distance vision.6
Click here for Important Product Information
Customizing the Approach to Presbyopia Management
Over the years, advancements in cataract surgery technology have made the operation relatively safe and more accurate, with outcomes more predictable for a wider array of patients. Improved diagnostics yield improved biometric measurements that translate in to more accurate power calculation. Coupled with refinements in surgical techniques and technology and strategies to optimize the ocular surface, surgeons now have at their disposal a full complement of tools to design a surgical plan likely to return patients to their desired activities after surgery—and at the core of this endeavor are new IOL options that simultaneously address presbyopia at the time of cataract surgery.
With the ReSTOR +2.5 IOL with ACTIVEFOCUS optical design, patients have the potential to achieve excellent distance vision with potentially fewer visual disturbances while performing distance tasks; in addition, they can reasonably expect to have functional vision at intermediate distances, and there is also a very good chance of spectacle independence for many daily activities due to the unique design of the ACTIVEFOCUS optic.1 As a result, surgeons are empowered with a new way of approaching cataract surgery, wherein they can work with each patient to understand his or her unique needs for postcataract surgery vision and plan corrections to the optical system accordingly.
In addition to the ReSTOR +2.5 IOL, the AcrySof IQ ReSTOR +3.0 Multifocal Toric, which gained approval in late 2016 and is available in spherical equivalent powers from +6.00 D to +30.00 D in 0.50 D steps. It is designed to correct astigmatism and is for patients who desire increased spectacle independence. The AcrySof IQ ReSTOR +2.5 Multifocal Toric IOL is also available and includes the ACTIVEFOCUS optical design. Together, these advanced additions to the growing family of AcrySof IQ IOLs mean that more patients can potentially achieve a high-quality refractive outcome after their cataract surgery, in turn raising the potential to truly customize the approach to vision correction.
Ultimately, in this new era of cataract surgery, setting a patient up for postoperative success hinges on selecting an IOL that provides the best chance of achieving the vision he or she wants. If the importance of understanding a patient’s visual demands based on lifestyle is crucial to delivering satisfaction, then the expanded options in IOLs affords the surgeon the ability to consider patients who previously may not have been candidates for presbyopia correction at the time of cataract surgery.
AcrySof IQ ReSTOR Family of IOLs Important Product Information
CAUTION: Federal (USA) law restricts this device to the sale by or on the order of a physician.
INDICATIONS: The AcrySof® IQ ReSTOR® Posterior Chamber Intraocular Multifocal IOLs include AcrySof IQ ReSTOR and AcrySof ReSTOR Toric and are intended for primary implantation for the visual correction of aphakia secondary to removal of a cataractous lens in adult patients with and without presbyopia, who desire near, intermediate and distance vision with increased spectacle independence. In addition, the AcrySof IQ ReSTOR Toric IOL is intended to correct pre-existing astigmatism. The lenses are intended to be placed in the capsular bag.
WARNINGS/PRECAUTIONS: Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/benefit ratio before implanting a lens in a patient with any of the conditions described in the Directions for Use labeling for each IOL. Physicians should target emmetropia, and ensure that IOL centration is achieved. Care should be taken to remove viscoelastic from the eye at the close of surgery.
The ReSTOR Toric IOL should not be implanted if the posterior capsule is ruptured, if the zonules are damaged, or if a primary posterior capsulotomy is planned. Rotation can reduce astigmatic correction; if necessary lens repositioning should occur as early as possible prior to lens encapsulation.
Some patients may experience visual disturbances and/or discomfort due to multifocality, especially under dim light conditions. A reduction in contrast sensitivity may occur in low light conditions. Visual symptoms may be significant enough that the patient will request explant of the multifocal IOL. Spectacle independence rates vary; some patients may need glasses when reading small print or looking at small objects.
Posterior capsule opacification (PCO), when present, may develop earlier into clinically significant PCO with multifocal IOLs. Prior to surgery, physicians should provide prospective patients with a copy of the Patient Information Brochure available from Alcon informing them of possible risks and benefits associated with the AcrySof® IQ ReSTOR® IOLs.
Do not resterilize; do not store over 45° C; use only sterile irrigating solutions such as BSS® or BSS PLUS® Sterile Intraocular Irrigating Solutions.
ATTENTION: Reference the Directions for Use labeling for each IOL for a complete listing of indications, warnings and precautions.
AcrySof, ACTIVEFOCUS, and ReSTOR are trademarks of Novartis. © Novartis 2017. All other brand/product names are the trademarks of their respective owners.
1. AcrySof IQ ReSTOR +2.5 Multifocal IOL Directions for Use.
2. Vega F, Alba-Bueno F, Millan MS, et al. Halo and through-focus performance of four diffractive multifocal intraocular lenses. Invest Ophthalmol Vis Sci. 2015:56(6):3967-3975.
3. Alcon Data on File (11 Apr 2016).
4. Alcon Data on File (18 Jul 2016).
5. Survey of 90 surgeons who implant a presbyopia correcting IOL. Brand Health Tracker. Conducted December 2015 and July 2016.
6. Nuijts RM, Jonker SM, Kaufer RA, et al. Bilateral implantation of +2.5 D multifocal intraocular lens and contralateral implantation of +2.5 D and +3.0 D multifocal intraocular lenses: clinical outcomes. J Cataract Refract Surg. 2016;42(2):194-202.
© 2017 Novartis 7/17 US-RES-17-E-1182l


