
The EVO ICL lens (EVO) opens refractive surgery up to a huge patient population. In addition to two full-thickness peri-optic ports and two full-thickness ports on the footplates, EVO has a novel 0.36-mm central port (Figure 1) that effectively allows physiologic aqueous flow. This results in an exceedingly low risk of pupillary block and anterior subcapsular cataract and eliminates the requirement for a preoperative peripheral iridotomy.1 Because aqueous can flow through the anterior segment and nourish the crystalline lens, IOP is well controlled while maintaining the quality of vision patients experience with this lens. Long-term evidence has shown that visual quality is excellent in eyes with moderate to high myopia.2 Now, current evidence also shows that EVO is an effective treatment for as low as -3.00 D of myopia.3
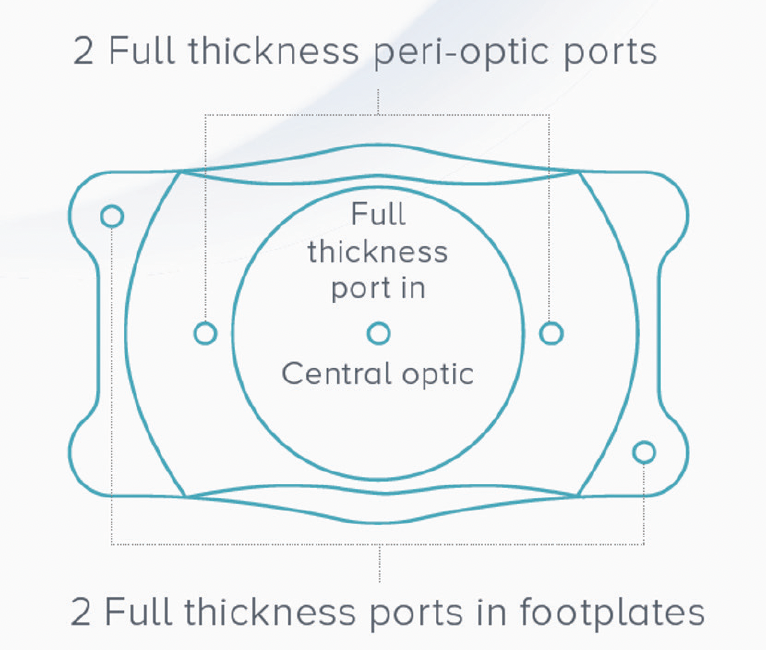
Figure 1. EVO uses advanced technology to provide outstanding safety.
Our experience has taught us that, regardless of the amount of refractive error, nailing the preoperative examination is the first step in achieving excellent outcomes with EVO.
MEASUREMENTS AND SIZING
Following a precise and straightforward preoperative evaluation process will help eliminate the outliers and enhance surgeon confidence in the EVO procedure. The preoperative exam for EVO is like any refractive surgical evaluation. The ocular surface, crystalline lens, iris, and retina are assessed. For EVO, the anterior chamber depth (ACD) is then measured with a device such as the Pentacam (Oculus). EVO is indicated for an ACD (true ACD) of 3.0 mm or greater. Additionally, we like to use ultrasound biomicroscopy (UBM) to look for iris or ciliary body cysts and anterior segment OCT to assess sulcus-to-sulcus measurement.
EVO sizing affects the vault, which should be approximately 250 to 900 µm.4 The standard method for ICL sizing is to obtain white-to-white measurements and import them into STAAR’s online calculator and ordering system (https://ocos.staar.com/). Another alternative is sulcus-to-sulcus measurements.
We use several devices to help with sizing, including the IOLMaster (Carl Zeiss Meditec), Lenstar (Haag-Streit), and Visante (Carl Zeiss Meditec). Note that it is not an FDA requirement to obtain multiple measurements. The basic requirement for sizing, according to the US FDA, is white-to-white diameter. All you need to feel comfortable picking a size for EVO is a single reliable way to look at white-to-white (or sulcus-to-sulcus) and anterior chamber depth. Having other diagnostic equipment available is helpful but by no means necessary.
SURGICAL TIPS FOR EVO
The surgical skill set required for cataract surgery converts into EVO surgery easily—much easier than phacoemulsification to LASIK. If you’re a careful, delicate cataract surgeon and can do a smooth procedure, then you can be an awesome ICL surgeon after completing the EVO certification training. For beginning surgeons, visit a surgeon who has a meticulous surgical technique with EVO or watch a surgical video of somebody who has a simple and predictable technique from start to finish. Our cornea/refractive surgery fellows at the University of Pittsburgh are certified to perform EVO surgery, and their results starting with their first case are the same as more experienced surgeons since they adopt the same technique. Our four top tips are the following.
- No. 1: The angle of the paracenteses is critically important. Angle the first paracentesis toward the leading footplates so the tucking step will be easier.
- No. 2: Manipulate the footplates into the correct position. Tuck the footplates with your instrument behind the iris gently but intentionally. We like the Battle ICL Manipulator (ASICO), for example.
- No 3. Consider the use of the Lioli injector (AST Products). This system allows us to inject EVO through a small incision, and there is much less manipulation during loading.
- No. 4: Be OCD about the OVD to avoid IOP spikes. We use OcuCoat (Bausch + Lomb), as recommended by STAAR, which is a low molecular weight HPMC. After EVO is implanted and in the correct orientation, we use balanced salt solution to begin the removal of the OVD from the anterior chamber. We then use bimanual irrigation and aspiration to finish the job. Using a meticulous but gentle technique can reduce the risk of cortical changes on the crystalline lens.
VAULT
In reality—with EVO—the vault is very forgiving. This doesn’t mean we shouldn’t measure the vault or pay attention to it, but selecting a lower vault, when appropriate, should not be concerning. The occurrence of cataract with the current model is rare. There were no cases (0.0%) of anterior subcapsular cataract in the US FDA clinical trial for EVO at 6 months and none reported in a review of the worldwide literature covering 4,196 eyes implanted with EVO lenses.3,5
CONCLUSION
Preoperative measurements are important for sizing EVO properly. With practice and the right strategy (for more surgical tips, see the sidebar above), it becomes easier to nail the intended outcome and provide patients with the best opportunity for superb vision after surgery.
1. Packer M. Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six month results from the United States Food and Drug Administration clinical trial. Clinical Ophthalmology. 2022;16:1541-1553.
2. Niu L, Miao H, Tian H, Ding L, Wang X, Zhou X. Visual outcomes of Visian ICL implantation for high myopia in patients with shallow anterior chamber depth. BMC Ophthalmol. 2019;19:121.
3. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
4. Alfonso JF, Fernandez-Vega L, Lisa C, et al. Central vault after phakic intraocular lens implantation: Correlation with anterior chamber depth, white-to-white distance, spherical equivalent, and patient age. J Cataract Refract Surg. 2012;38:46-53.
5. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427-2438.

