
In recent years, I have embraced a procedure for a formerly overlooked and undertreated pathology. In just under 5 years, I have performed more than 3,000 laser floater removal (LFR) procedures, excising impediments to clear vision and inspiring gratitude in a cohort of patients.
Treating floaters has not been a priority for a variety of reasons, chief among them, lack of technology specifically designed for visualizing the vitreous. Previous lasers did not provide an appropriate illumination source to effectively view the mid- and posterior vitreous (where the bulk of symptomatic floaters reside), resulting in a lack of spatial context. We also lacked a laser that provided a safe energy delivery profile. These factors negatively weighted the risk-benefit ratio, resulting in floater treatment being placed on the proverbial low-to-no-priority list.
New Technology
The risk/benefit ratio has greatly improved since the introduction of Reflex Technology (Ellex). Reflex Technology supplants older YAG laser technology by offering effective treatment of opacities throughout the entire vitreous cavity. The Tango Reflex and Ultra Q Reflex systems (Ellex) provides True Coaxial Illumination (TCI), which means the illumination tower, the oculars, and the laser beam are all on the same optical pathway facilitating visualization of the floater and the retina at the same time. With coaxial illumination, we have a better understanding of where we are in the vitreous when performing LFR. For instance, if the floater is in focus at the same time as the retina, it is not safe to fire because the floater is too close to the retina. Conversely, if the floater is in focus and the retina is out of focus, or not seen at all, we are safe to fire because the floater is far enough away from the retina. Moreover, the laser system has been designed to deliver energy with more efficiency, which results in a decreased likelihood of collateral damage. Both the Tango Reflex and Ultra Q Reflex feature an energy profile of a narrow ultra-Gaussian, 4-nanosecond beam that has a fast pulse rise and fall time and small spot size. Using this new laser technology, along with a new midvitreous lens that further improves visualization, enables us to better answer the question, “is it worth treating?” The answer is now a resounding, “yes.” The laser energy profile and enhanced visualization provided by TCI minimize the risk and leave us with an opportunity to provide the benefit of improved quality of vision and quality of life to our patients. Once I performed multiple LFR procedures, it became clear that the impact of the procedure on patients was significant—often similar to postoperative cataract patients who are relieved and excited at the prospect of once again being able to perform daily functions such as reading or driving.
Case Studies
Not all floaters are the same; there are those that are tiny dots and others that are fine strings; these floaters tend to be less bothersome (but harder to treat). Then there are large Weiss rings and amorphous clumps—like a large cloud in the middle of the vitreous, which tend to interfere with daily functioning. Now, by paying more attention to the vitreous, I am seeing the prevalence of these larger floaters increasing in my clinic. In fact, many of these patients present complaining of a “shadow” in their vision, often similar to those describing a scotoma.
One of these cases, in particular, stands out. A 54-year-old man came in for a consultation after seeing two other optometrists and an ophthalmologist. He presented to me complaining of a large blur in his front vision that was fairly dense and would interfere with many of his daily tasks. I identified a large amorphous floater in the middle-to-posterior vitreous approximately 3 millimeters away from the retina. Upon examination, I noticed that the floater had a large U shape similar to what the patient described, and this was confirmed on optical coherence tomography (OCT), as well. OCT showed a large, amorphous, U-shaped opacity that was also causing a shadow on the corresponding retinal 5-line raster scans (Figure 1).
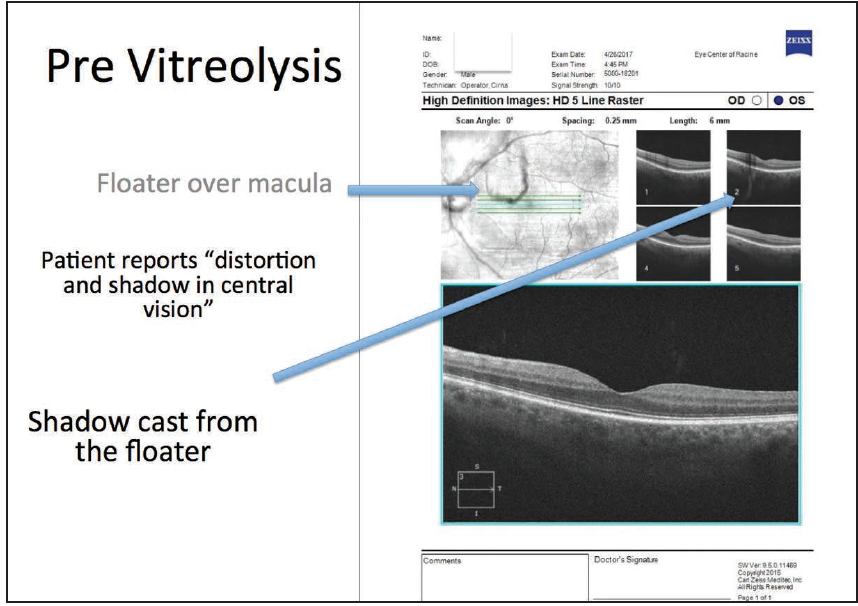
Figure 1. OCT showed a large, amorphous, U-shaped opacity.
We deemed this U-shaped floater a clinically significant vitreous opacity and decided that it warranted removal. We discussed the reasons for his etymology with the patient, recommended LFR, and scheduled his first session.
We used the Singh midvitreous lens (Volk) with the Ellex Ultra Q Reflex laser system, featuring TCI, and performed the treatment using 6 mJ with a total of 685 laser shots. We were able to vaporize the majority of the floater, leaving just the two top ends of the U shape. I refrained from attempting to vaporize those remaining pieces, because they were too close to the retina, and we had already fired nearly 700 shots. Postoperatively, the vast majority of the floater was gone on slit-lamp examination, and more importantly, the shadow on the retina was gone on the postoperative OCT scan as well (Figure 2).
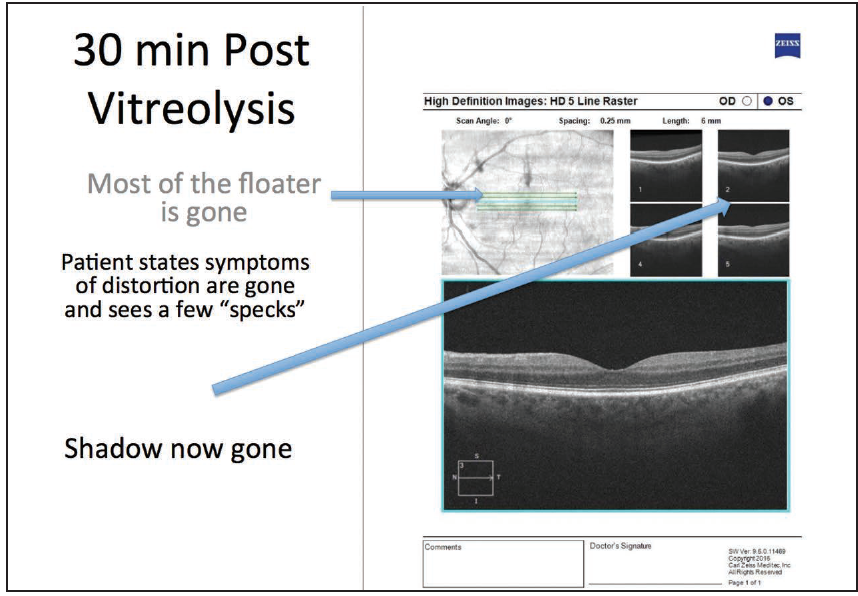
Figure 2. Postoperative OCT shows shadow is gone.
In a similar case, a 47-year-old woman presented with complaints of loss of central vision in her right eye. After a detailed history, she described a “blurry shadow” that would not move out of her central vision. She had been to an optometrist and an ophthalmologist who had not identified the source of her problem. She had become so distraught that she eventually underwent magnetic resonance imaging and electroencephalograms, and once again, nothing was found. She came to our office and after finding nothing upon examination, our optometrist called me into the room to see the patient. A quick look under the slit lamp immediately revealed a large amorphous cloud-like floater in the middle of her vitreous, right over the fovea.
We subsequently ordered two separate macular OCTs (on different days), which both demonstrated the same large opacity in the vitreous, which did not move. There was also a shadow cast on the retina corresponding to the floater, which explained her symptoms. We scheduled a LFR procedure, which I performed shortly after the consult. Following the procedure, we performed a postoperative OCT; the larger opacity was gone, as was the shadow cast on the retina. More importantly, the patient also described resolution of her symptoms.
Take-Home Message
Many of us miss vitreous opacities and do not commonly look at the vitreous as a cause of our patients’ quality of vision complaints. We are not often trained to focus on the vitreous; we usually pay close attention to the cornea, lens, nerve, and retina, but often overlook the largest part of the eye, the vitreous, which, of course, serves as a crucial component of the optical system.
Now that I have performed thousands of these LFR cases, I routinely take time to look at the vitreous in all my patients. I find many more floaters than I used to, primarily because I am looking for them. It is like any other skill; once you train your mind to look for these opacities, it becomes easier to find them.
I have learned several things from these types of cases: first, floaters can impact visual acuity and visual quality; second, clinically significant symptomatic opacities often compromise visual function, and that ultimately negatively impacts quality of life by precluding participation in routine daily activities, and the availability of this new Reflex YAG laser makes it possible for me to give my patients back the ability to enjoy these activities; and third, OCTs are not only useful for viewing the macular contour and layers, they can be used to evaluate the effect of a floater by visualizing the shadow that it casts on the macula. Finally, and perhaps the most important thing I have learned is that the availability of this new Reflex Technology provides an affirmative response to the question, “is it worth treating?” The coaxial illumination system and truncated laser energy profile mitigate the risk of the procedure, and therefore allow us to finally offer a safe and effective opportunity to help these suffering patients.