
A crucial aspect of delivering patients the postoperative outcome they want is ensuring the vision will last long-term. Thus, the stability of the refractive outcome is an important aspect to consider in cataract surgery.
The AcrySof IQ ReSTOR IOL (Alcon) platform has been specifically engineered to deliver unrivaled stability. Within the family of lenses, this stability has different but equally important implications for the toric model and the +2.5 and +3.0 models designed to provide a full range of vision with uncompromised distance. 1-3
Stability in Astigmatism Correction
Toric IOLs can be a highly effective option for correcting astigmatism at the time of cataract surgery. However, improper alignment and postoperative rotation of the toric IOL are both risk factors for less than ideal astigmatism correction.
Proper alignment of a toric IOL is often a byproduct of careful preoperative planning and meticulous surgery. On the other hand, rotational stability of a toric IOL is largely a function of the lens design—and in this regard, the AcrySof IQ Toric IOL with ACTIVEFOCUS provides better refractive predictability and stability compared with other on-market options. Compared with other toric models that use an offset haptic design4 that may be prone to hyperopic shift5 and have a propensity for counterclockwise rotation,6 the profile of the AcrySof ReSTOR Toric IOL7 has been designed to provide excellent rotational stability7-11 with no rotational bias.6
While these features are technically interesting and provide the best conditions to reduce axial rotation, their importance in clinical settings is supported by data from registries and clinical trials. An analysis of over 5,000 surgeries involving two leading toric IOLs found that the AcrySof IQ Toric IOL was less likely to rotate 5° or greater off axis. Overall, the AcrySof IQ Toric was 5º or more off axis in 0.75% of cases (n = 3,556) compared to 1.86% with a competitor lens (n = 1,953).6 As there is seemingly less margin for error in astigmatism correction, this becomes crucial for ensuring both quantity and quality of postoperative vision (Figure 1).
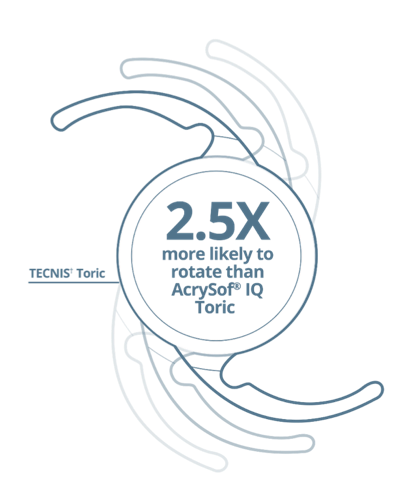
Figure 1. The propensity for other toric IOL models to rotate counterclockwise has also been noted in direct head-to-head comparison studies.12
The propensity for other toric IOL models to rotate counterclockwise has also been noted in direct head-to-head comparison studies.12 In a series of over 1,200 cases, Lee and Chang also noted that the AcrySof IQ Toric IOL was more consistently within 5° of the intended axis on the first postoperative visit (91.9% of cases compared to 81% with another toric model).12 The study noted a mean rotation of 2.72° associated with the AcrySof IQ Toric IOL versus 3.79° and a trend toward lower need for secondary repositioning associated with the AcrySof IQ Toric IOL.
Reducing the Potential for Refractive Surprises
The stability of the refractive result is equally important for all cataract surgery patients, regardless of whether a toric implant is used. One notable feature of the AcrySof IQ ReSTOR IOL platform is that it is constructed of a highly biocompatible material that supports fibronectin binding, thereby providing the conditions for excellent capsule adhesion.13,14 This is no small consideration given to the potential to reduce the need for postoperative revision.15,16
The addition of the ACTIVEFOCUS design to the AcrySof IQ ReSTOR IOL platform technology provides additional properties that help avoid refractive surprises in the postoperative period. Because the central vision zone is 100% dedicated to distance, the lens is less sensitive to decentration that might otherwise negatively affect contrast sensitivity (Figure 2).17
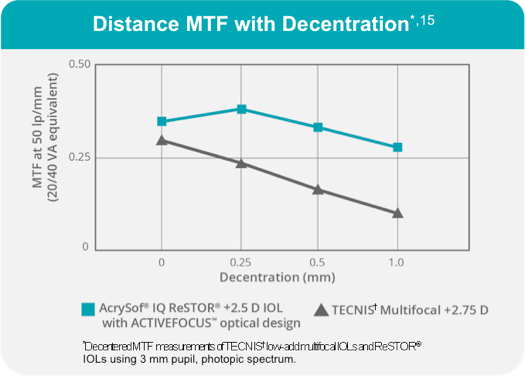
Figure 2. The AcrySof +2.5 IOL maintains its modular transfer function score, a measure of the lens’ ability to preserve original contrast,18 through 0.5 mm of decentration.
Conclusion
Achieving the final vision that patients want involves several overlapping variables. We can work closely with patients to identify their goals and tailor the surgical plan toward providing vision that allows them to return to their active lifestyles. Meanwhile, careful preoperative planning and meticulous cataract surgery contribute to less traumatic operations that reduce the potential for iatrogenic trauma. Yet, there is still a risk of a postoperative refractive surprise in the case of axial misalignment or if the IOL placement is not maintained after surgery.
With the understanding that many cataract patients want to resume active lifestyles after surgery—and indeed, this is a prime reason many patients opt for presbyopia- and astigmatism-correcting IOL options—the modern cataract surgeon is tasked with providing excellent quantity and quality of vision. The ability to deliver on that expectation is greatly facilitated by lens designs that help lock down the visual outcome so patients can enjoy their postoperative vision long-term.
AcrySof, ACTIVEFOCUS, and ReSTOR are trademarks of Novartis. © Novartis 2018. All other brand/product names are the trademarks of their respective owners.
1. Alcon Data on File (April 11, 2016).
2. AcrySof® IQ ReSTOR® +2.5 D IOL Directions for Use.
3. Vega F, Alba-Bueno F, Millán MS, Varon C, Gil MA, Buil JA. Halo and through-focus performance of four diffractive multifocal intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(6):3967-3975 (study conducted with corneal model eye with 0.28μ spherical aberration).
4. TECNIS* Toric Aspheric IOL Specification Sheet. Abbott Medical*, 2015.
5. Eldaly MA, Mansour KA. Personal A-constant in relation to axial length with various intraocular lenses. Indian J Ophthalmol. 2014;62(7):788-791.
6. Potvin R, et al. Toric intraocular lens orientation and residual refractive astigmatism: an analysis. Clin Ophthalmol. 2016;10:1829-1836.
7. AcrySof® IQ Toric IOL Directions for Use.
8. Wirtitsch MG, et al. Effect of haptic design on change in axial lens position after cataract surgery. J Cataract Refract Surg. 2004;30(1):45-51.
9. Nejima R, et al. Prospective intrapatient comparison of 6.0-millimeter optic single-piece and 3-piece hydrophobic acrylic foldable intraocular lenses. Ophthalmology. 2006;113(4):585-590.
10. Lane SS, Ernest P, Miller KM, Hileman KS, Harris B, Waycaster CR. Comparison of clinical and patient reported outcomes with bilateral AcrySof® Toric or spherical control intraocular lenses. J Refract Surg. 2009;25(10):899-901.
11. Lane SS, Burgi P, Milios GS, Orchowski MW, Vaughan M, Schwarte E. Comparison of the biomechanical behavior of foldable intraocular lenses. J Cataract Refract Surg. 2004;30:2397-2402.
12. Lee BS, Chang DF. Comparison of the Rotational Stability of Two Toric Intraocular Lenses in 1273 Consecutive Eyes. Ophthalmology. 2018 Mar 12. pii: S0161-6420(17)33524-8. doi: 10.1016/j.ophtha.2018.02.012. [Epub ahead of print]
13. Ong M, Wang L, Karakelle M. Fibronectin adhesive properties of various intraocular lens materials. Invest Ophthalmol Vis Sci. 2013;54(15):819-B0043.
14. Linnola RJ, Sund M, Ylonen R, et al. Adhesion of soluble fibronectin, laminin, collagen type IV to intraocular lens materials. J Cataract Refract Surg. 1999;25(11):1486-1491.
15. Boureau C, et al. Incidence of Nd:YAG laser capsulotomies after cataract surgery: comparison of 3 square edge lenses of different composition. Can J Ophthalmol. 2009;44:165-170.
16. Apple DJ, Peng Q, Visessook N, et al. Eradication of posterior capsule opacification: documentation of a marked decrease in Nd:YAG laser posterior capsulotomy rates noted in an analysis of 5,416 pseudophakic human eyes obtained postmortem. Ophthalmology. 2001;108(3):505-518.
17. Alcon Data on File (Oct 6, 2016).
18. Hill W. Modulation Transfer Function (MTF). East Valley Ophthalmology website. https://doctor-hill.com/patients/modulation_transfer_function.htm. Accessed Feb. 2, 2018.



AcrySof® IQ ReSTOR® Family of Multifocal IOLs Important Product Information
CAUTION: Federal (USA) law restricts this device to the sale by or on the order of a physician.
INDICATIONS: The AcrySof® IQ ReSTOR® Posterior Chamber Intraocular Multifocal IOLs include AcrySof® IQ ReSTOR® and AcrySof® IQ ReSTOR® Toric and are intended for primary implantation for the visual correction of aphakia secondary to removal of a cataractous lens in adult patients with and without presbyopia, who desire near, intermediate and distance vision with increased spectacle independence. In addition, the AcrySof® IQ ReSTOR® Toric IOL is intended to correct pre-existing astigmatism. The lenses are intended to be placed in the capsular bag.
WARNINGS/PRECAUTIONS: Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/benefit ratio before implanting a lens in a patient with any of the conditions described in the Directions for Use labeling for each IOL. Physicians should target emmetropia, and ensure that IOL centration is achieved. Care should be taken to remove viscoelastic from the eye at the close of surgery.
The ReSTOR Toric IOL should not be implanted if the posterior capsule is ruptured, if the zonules are damaged, or if a primary posterior capsulotomy is planned. Rotation can reduce astigmatic correction; if necessary lens repositioning should occur as early as possible prior to lens encapsulation.
Some patients may experience visual disturbances and/or discomfort due to multifocality, especially under dim light conditions. A reduction in contrast sensitivity may occur in low light conditions. Visual symptoms may be significant enough that the patient will request explant of the multifocal IOL. Spectacle independence rates vary; some patients may need glasses when reading small print or looking at small objects.
Posterior capsule opacification (PCO), when present, may develop earlier into clinically significant PCO with multifocal IOLs. Prior to surgery, physicians should provide prospective patients with a copy of the Patient Information Brochure available from Alcon informing them of possible risks and benefits associated with the AcrySof® IQ ReSTOR® IOLs.
Do not resterilize; do not store over 45° C; use only sterile irrigating solutions such as BSS® or BSS PLUS® Sterile Intraocular Irrigating Solutions.
ATTENTION: Reference the Directions for Use labeling for each IOL for a complete listing of indications, warnings and precautions.
© 2018 Novartis 8/18 US-RES-18-E-1855