
With the advancement in cataract IOL technology, we now have more options than ever to help mitigate presbyopia in our cataract patients. Based on our patients' ocular health, lifestyle, and expectation, we can offer IOLs ranging from monofocals for excellent distance vision, to non-diffractive extended depth of focus (EDOF) IOLs for added intermediate and functional near vision, to full range of vision IOLs (eg, trifocals) for patients who desire a greater level of spectacle independence and are willing to accept some nighttime visual disturbances.1-3 To meet the increasingly high demand from modern day cataract patients, it is critical for us, the ophthalmic surgeons, to have a solid understanding of the current IOL technologies and their real-world clinical outcomes to provide the best education and IOL recommendation to our patients.
PanOptix®, the first US FDA approved trifocal lens, has become the most implanted trifocal IOL in the world since its initial usage in Europe almost 10 years ago.4,5 PanOptix® employs a unique ENLIGHTEN technology to enhance light energy usage and provide three focal points for distance, intermediate and near. One distinct feature that differentiates PanOptix® from other traditional trifocal IOLs is the 60 cm intermediate focal point, which allows comfortable arm's length activity for the average height person.6
Since its launch, ophthalmologists around the world have utilized PanOptix® IOLs and reported their experiences in more than 150 peer-reviewed articles. Literature reviews to summarize the PanOptix® IOLs clinical performance help us to have an easy and better understanding of its real-world performance.
A worldwide pooled efficacy and safety analysis recently conducted by Dr. Kohnen et al. included six PanOptix® clinical trials conducted in the US and various countries across Europe, Australia, Asia and South America in cataract patients from different ethnicities and cultural backgrounds.7 The study showed that bilateral implantation of PanOptix® consistently provided 20/20-2 vision at distance, intermediate and near. The pooled PanOptix® binocular defocus curve demonstrated a continuous range of vision of 20/25 or better from distance to near (33 cm) (Figure 1).
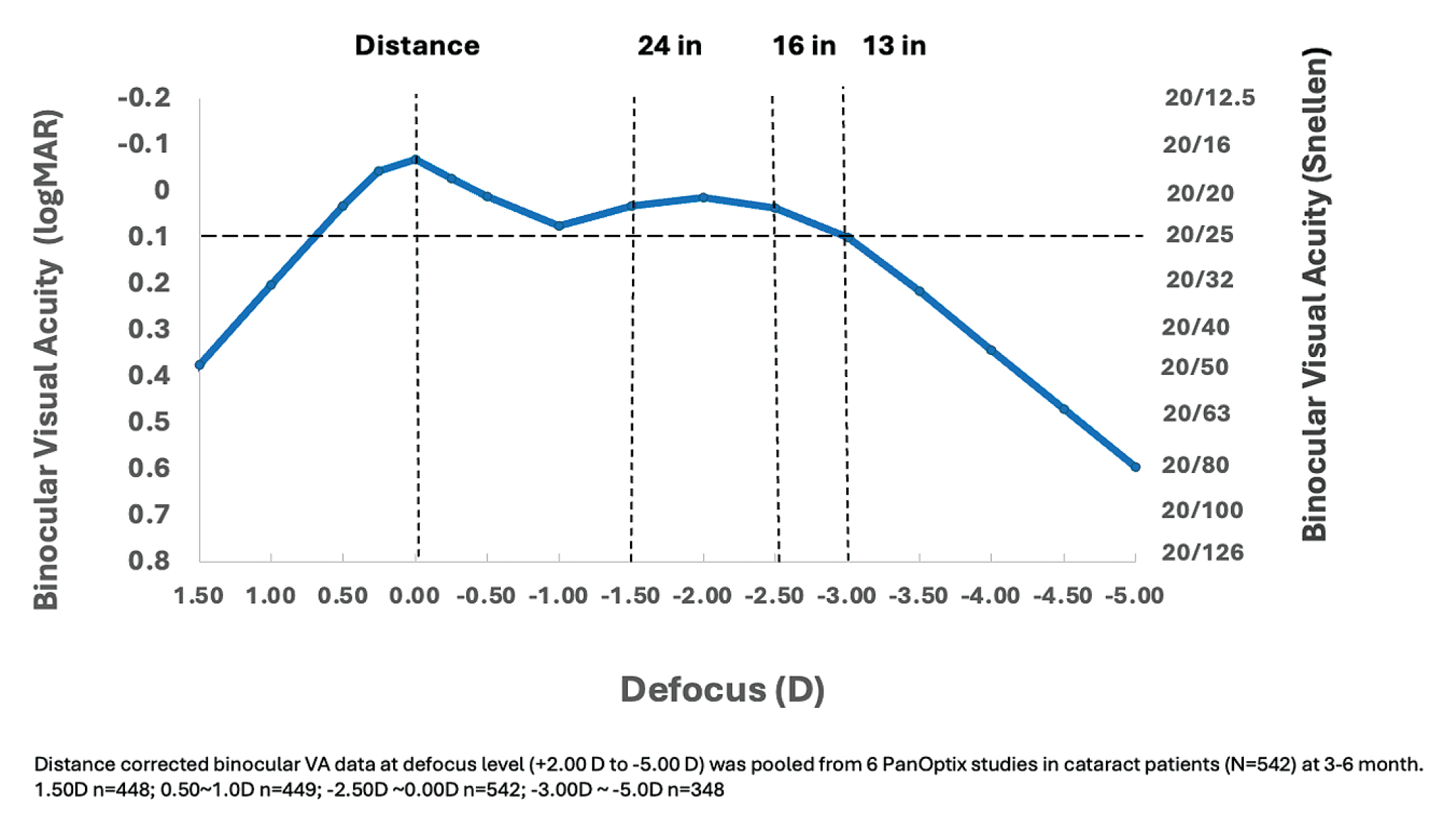
Figure 1. The PanOptix® binocular defocus curve, pooled from six PanOptix® studies in cataract patients.
Ocular adverse effects associated with PanOptix® implantation were extremely low; the most frequently reported were halos at 2.2% and 2% and glare at 1.1% and 0.9% in the first (n=557) and second eye (n=547), respectively. There were four reported secondary surgical interventions with two explants due to blurred vision and two IOL repositionings.7
In collaboration with Alcon, we recently conducted two systemic literature reviews and meta-analyses to calculate the overall patient-reported complete spectacle independence8 and patient-reported unwanted visual phenomena9 after bilateral PanOptix® implantation.
Consistent with the PanOptix® adverse events found in the above pooled analysis, the meta-analysis of patient-reported visual phenomena in those peer-reviewed articles published between April 2021 and December 2022, and those unpublished clinical studies presented at major conferences in 2021 and 2022, showed that the most frequently reported visual phenomena are glare, halos and starbursts9 (Figure 2). Eleven randomized controlled trials or observational clinical studies that described patient-reported visual disturbances at least 1 month after bilateral AcrySof IQ PanOptix®/PanOptix® toric IOL implantation were identified. Fixed and random effects meta-analyses were conducted. Pooled proportion for the three most frequently patient-reported visual disturbances (glare, halos and starbursts), were calculated (Figure 2).

Figure 2. Meta-analysis summary of visual disturbance estimates after cataract surgery with bilateral implantation of AcrySof IQ PanOptix®/PanOptix® toric IOLs.9
Based on this data, we can tell our patients that approximately 5% of cataract patients may experience “severe” visual disturbances, glare, halos and starbursts, and less than 3% of patients may experience "very bothersome” visual disturbances after bilateral implantation of PanOptix® IOLs.9
In the separate meta-analysis analyzing spectacle independence,8 we reviewed the published clinical studies on AcrySof IQ PanOptix® and PanOptix® toric IOLs listed in PubMed from 2017 to September 2021 and the relevant completed but unpublished studies presented in major ophthalmic conferences up to 2021. Thirteen unique clinical studies that reported complete spectacle independence (SI) after bilateral PanOptix® or PanOptix® toric IOL implantation in cataract patients (n= 513) were included in the base-case Bayesian random-effects meta-analysis. The complete SI rate was 91.6%. Three subgroup analyses from 13 studies (n=603 patients) showed that the rate of SI for far, intermediate and near vision were 95.9%, 96.3% and 89.6%, respectively.
Overall, this meta-analysis demonstrated that at least 9 out of 10 patients receiving AcrySof IQ PanOptix® IOL during cataract surgery can expect to achieve complete spectacle independence.8
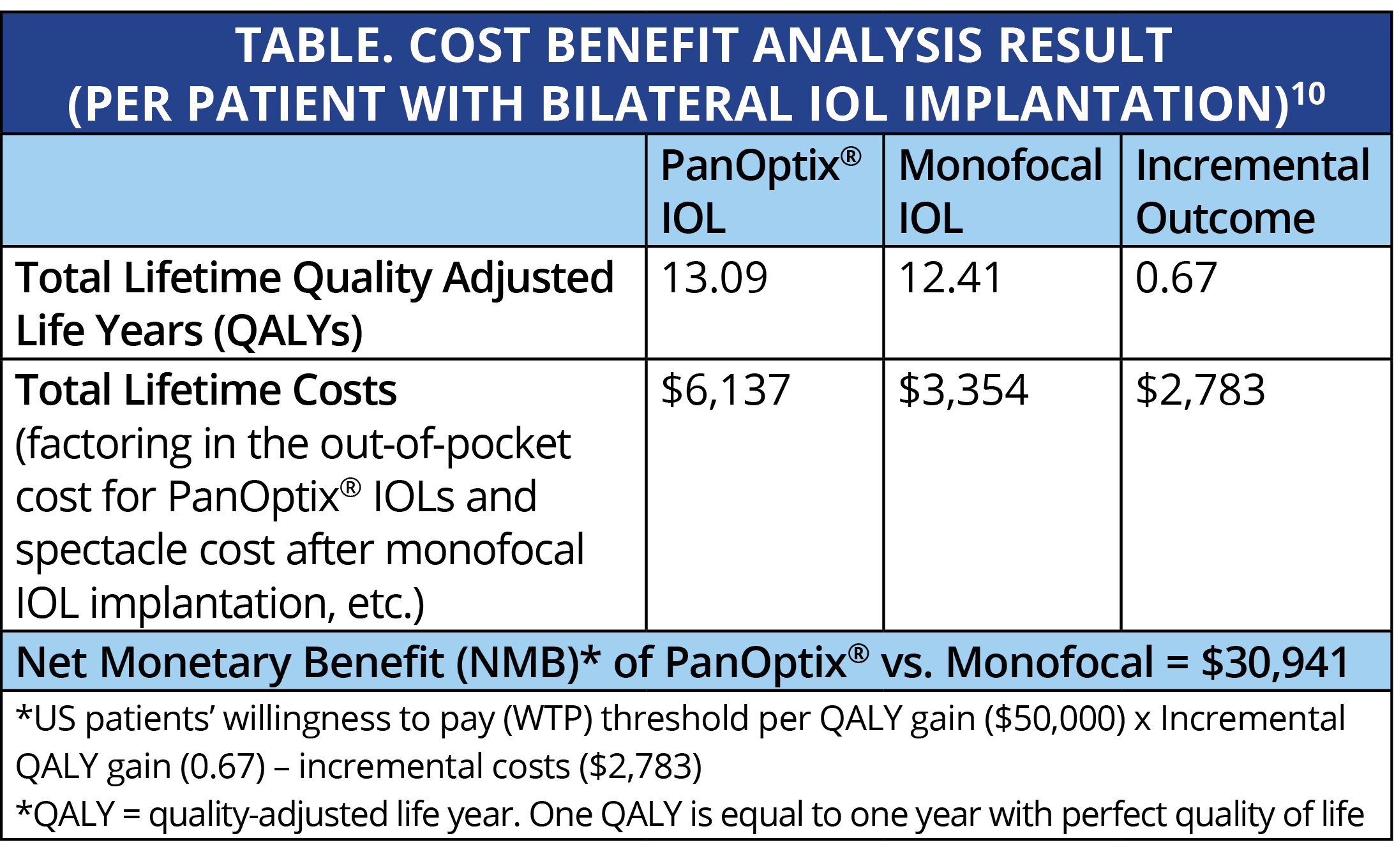
The presbyopia correcting IOL adoption rate has remained low for many years even with the significant advancement of IOL technology. One major concern from cataract patients is the relatively high one-time out of pocket cost. Berdahl et al10 performed an enlightening cost-benefit analysis that should help us to communicate better with our potential PCIOL patients.
The study estimated the lifetime vision-related quality of life gains and costs that patients could expect from PanOptix® compared to a monofocal IOL. Factors affecting the vision related quality of life include post-operative spectacle dependence, risk of very bothersome visual disturbances (glare, halos, or starbursts), and the need for secondary surgical interventions. The study found that bilateral implantation of PanOptix® trifocal IOLs would have a lifetime gain of 0.67 QALYs* compared to patients with monofocal IOL implantation. Overall, this incremental QALY gain translated into a lifetime net monetary benefit of $30,941 at the patients' willingness to pay threshold of $50,000/QALY gain (Table).
Overall, PanOptix® provides cataract patients with great vision from distance to near with high spectacle independence.7,8 Compared to monofocal IOls, PanOptix® provides better vision related quality of life and is a cost-beneficial treatment strategy for cataract patients.10
AcrySof® IQ PanOptix® Family of Trifocal IOLs
IMPORTANT PRODUCT INFORMATION
CAUTION: Federal (USA) law restricts this device to the sale by or on the order of a physician.
INDICATIONS
The AcrySof® IQ PanOptix® Trifocal IOLs include AcrySof® IQ PanOptix® and PanOptix® Toric and are indicated for primary implantation in the capsular bag in the posterior chamber of the eye for the visual correction of aphakia in adult patients, with less than 1 diopter of pre-existing corneal astigmatism, in whom a cataractous lens has been removed. The lens mitigates the effects of presbyopia by providing improved intermediate and near visual acuity, while maintaining comparable distance visual acuity with a reduced need for eyeglasses, compared to a monofocal IOL. In addition, the AcrySof® IQ PanOptix® Toric Trifocal IOL is indicated for the reduction of residual refractive astigmatism.
WARNINGS/PRECAUTIONS: Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/benefit ratio before implanting a lens in a patient with any of the conditions described in the Directions for Use labeling. Physicians should target emmetropia, and ensure that IOL centration is achieved.
For the AcrySof® IQ PanOptix® Toric Trifocal IOLs, the lens should not be implanted if the posterior capsule is ruptured, if the zonules are damaged, or if a primary posterior capsulotomy is planned. Rotation can reduce astigmatic correction; if necessary lens repositioning should occur as early as possible prior to lens encapsulation.
Some visual effects may be expected due to the superposition of focused and unfocused multiple images. These may include some perceptions of halos or starbursts, as well as other visual symptoms. As with other multifocal IOLs, there is a possibility that visual symptoms may be significant enough that the patient will request explant of the multifocal IOL. A reduction in contrast sensitivity as compared to a monofocal IOL may be experienced by some patients and may be more prevalent in low lighting conditions. Therefore, patients implanted with multifocal IOLs should exercise caution when driving at night or in poor visibility conditions.
Patients should be advised that unexpected outcomes could lead to continued spectacle dependence or the need for secondary surgical intervention (e.g., intraocular lens replacement or repositioning).
As with other multifocal IOLs, patients may need glasses when reading small print or looking at small objects. Posterior capsule opacification (PCO), may significantly affect the vision of patients with multifocal IOLs sooner in its progression than patients with monofocal IOLs. Prior to surgery, physicians should provide prospective patients with a copy of the Patient Information Brochure available from Alcon informing them of possible risks and benefits associated with the AcrySof® IQ PanOptix® Trifocal IOLs.
ATTENTION: Reference the Directions for Use labeling for each IOL for a complete listing of indications, warnings and precautions.
1. McCabe C et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022 Nov 1;48(11):1297-1304.
2. Sudhir RR, et al. AcrySof IQ PanOptix Intraocular Lens Versus Extended Depth of Focus Intraocular Lens and Trifocal Intraocular Lens: A Clinical Overview. Asia Pac J Ophthalmol (Phila). 2019 Jul-Aug;8(4):335-349.
3. TECNIS Synergy DFU.
4. Alcon data on file (2022)
5. MARKET SCOPE – 2022 IOL Market Report
6. Kohnen T, et al. Visual Performance of a Quadrifocal (Trifocal) Intraocular Lens Following Removal of the Crystalline Lens. Am J Ophthalmol. 2017 Dec;184:52-62.
7. Kohnen T, et al. Clinical Outcomes After Bilateral Implantation of a Diffractive Trifocal Intraocular Lens: A Worldwide Pooled Analysis of Prospective Clinical Investigations. Clin Ophthalmol. 2023 Jan 10;17:155-163.
8. Zhu D, et al. Rate of Complete Spectacle Independence with a Trifocal Intraocular Lens: A Systematic Literature Review and Meta-Analysis. Ophthalmol Ther. 2023 Apr;12(2):1157-1171.
9. Zhu D, Zhang J. Patient-reported outcomes of visual disturbances with a trifocal intraocular lens: a meta-analysis. Paper presented at: American Society of Cataract and Refractive Surgery Annual Meeting; April 7, 2024; Boston, USA
10. Berdahl J, et al. (2022) Cost-benefit analysis of a trifocal intraocular lens versus a monofocal intraocular lens from the patient’s perspective in the United States. PLoS ONE 17(11): e0277093.
© 2024 Alcon Inc. 10/24 US-ACP-2400010
The views and opinions expressed here may not represent those of Bryn Mawr Communications or Cataract & Refractive Surgery Today.



