



We have witnessed a conceptual transfiguration in many ophthalmic surgical procedures over the past few decades. For example, the paradigm of cataract surgery has changed from a procedure with the purpose of restoring transparency to the lens to one with a refractive purpose. The accuracy and safety of modern cataract surgery have transformed our patients’ expectations and have also increased their awareness of postoperative side effects. To meet their expectations, refractive surgeons rely on technology to achieve accurate ocular measurements and to deliver a perfect surgical outcome.
With premium IOL procedures, it is crucial to evaluate patient satisfaction after surgery. As refractive surgeons, we must understand our patients’ perspectives. For example, patients are not interested in our refractive accuracy, but rather in their own happiness and satisfaction with their postoperative vision. If patients are satisfied with their visual results, then we have met their expectations. The best way to leverage our results and our patients’ satisfaction after surgery is to be proactive before surgery.
SCREENING BEFORE ANY PROCEDURE
In my clinic, patient selection starts even before any ocular examination. When we talk to patients at an initial consultation, we assess their personality types and their expectations regarding surgery. The red flags we look for regarding multifocal IOL candidacy are patients with high visual demands and those who are meticulous when describing their visual impairment. Such clues suggest that these patients might not adapt well to the visual compromises necessary with multifocal lenses.
After this first step, an advanced ocular analysis should be performed to assess optical quality and ocular health, especially for patients who desire to undergo refractive lens exchange.
RIGOROUS SLIT-LAMP EXAMINATION
Conducting a detailed slit-lamp examination is an indispensable art. The status of the tear film should be evaluated because the majority of postoperative patient complaints are related to dry eye disease (DED). To improve postoperative outcomes, it is crucial to exclude patients with severe DED and to treat these patients accordingly. In patients with mild to moderate DED, I prefer to manage the condition before considering any type of refractive surgery.
At the slit-lamp, I also check for iris defects, pupil motility, and zonular and capsular issues. This helps me to be aware of signs of pseudoexfoliation before going to the OR.
Patients should also be educated about floaters and vitreous detachment if either is observed on fundoscopy. These findings may be associated with greater visual disturbances in patients after multifocal IOL implantation, so they can be reasons to exclude a candidate preoperatively—especially in a patient with high myopia.
OCULAR SURFACE AND QUALITY CHECK
Ancillary exams are essential to our screening process, and the information and images generated can help us educate our patients. For example, Placido disc–based or LED topography can be used to further assess and classify the severity of DED (Figure 1). Scheimpflug and OCT imaging tools are useful to check (and recheck) corneal astigmatism and optical quality. I also evaluate the magnitude of higher-order aberrations, setting a cut-off value at 0.30 µm to rule out poor multifocal IOL candidates (Figure 2).
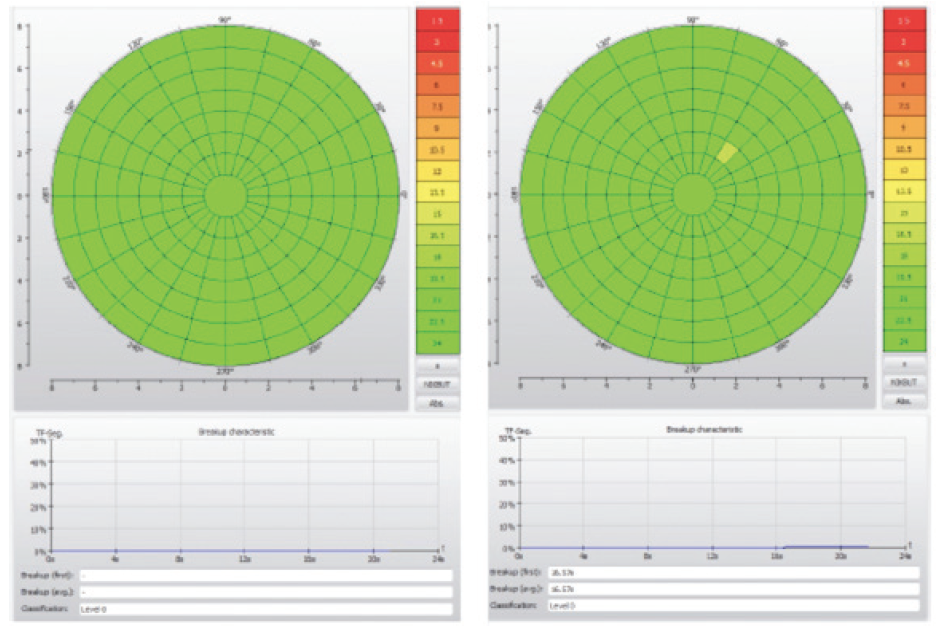
Figure 1. This scan with the Keratograph 5M (Oculus Optikgeräte) shows a regular and stable tear film in both eyes, with a tear film breakup time greater than 15 seconds.
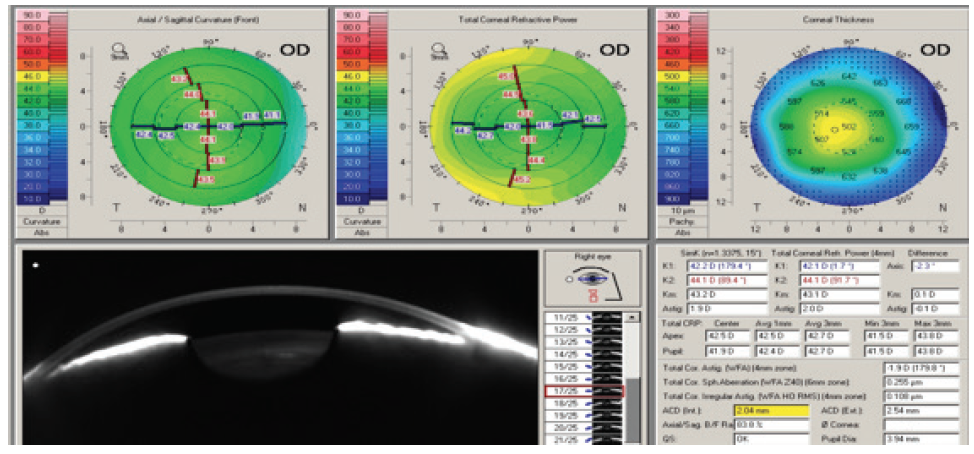
Figure 2. This clinical example using the Pentacam (Oculus Optikgeräte) presents a very low index of irregular astigmatism (0.108 μm). A toric lens will be needed because the patient has 2.00 D of total corneal astigmatism.
For success with multifocal IOLs, the cornea cannot present opacities or irregularities that compromise transparency. Therefore, specular microscopy must be used to assess the health of the endothelium. Patients with mild or forme fruste Fuchs dystrophy should be excluded from premium IOL candidacy because this condition may compromise corneal transparency postoperatively.
PREVIEW OF PERFECT CENTRATION
The success of multifocal IOLs depends on proper centration and implantation. When a premium IOL is decentered or tilted, it can result in a reduction of contrast sensitivity, induction of aberrations, and, consequently, decreases in visual acuity and patient satisfaction. I rely on the alpha angle parameter to optimize IOL centration on the visual axis in order to reduce complaints of dysphotopic effects.
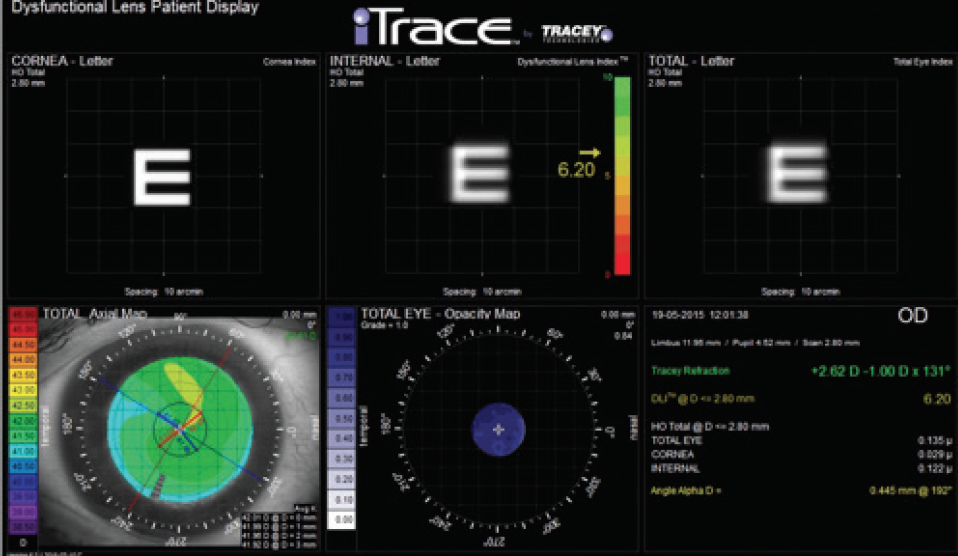
Figure 3. The dysfunctional lens display provided by the iTrace Visual Function Analyzer shows the corneal and crystalline lens contributions to the total eye vision. This display also provides data regarding the visual axes, specifically angle alpha.
There are several devices that measure parameters related to different visual axes. For example, the iTrace Visual Function Analyzer (Tracey Technologies) color-codes the amount of angle alpha, and I find this analysis useful for patient selection (Figure 3). An angle of 0.3 mm or less is coded green, 0.3 to 0.5 mm is coded yellow, and greater than 0.5 mm is coded red. Patients with a large angle alpha (>0.5 mm) should be excluded from premium IOL candidacy. In this condition, the optical axis of the multifocal IOL may not match the patient’s visual axis, leading to postoperative refractive surprises and dysphotopsia complaints.
RETINA STATUS CHECK
Macular function testing is another important part of our screening process. Visual acuity of 20/20 may not be enough to ensure postoperative satisfaction. OCT can provide macular and optic-disc analysis to look for subtle or occult pathology that could lead to decreased contrast sensitivity.
For example, I exclude patients who may experience postoperative progression of macular disease after cataract surgery, specifically those with macular degeneration, epiretinal membrane, or localized vitreoretinal traction. I also rule out patients with mild abnormalities in the optic nerve structure. If these abnormalities are significant and/or progressive, a multifocal IOL should be considered a contraindication to long-term success for these patients.
CONCLUSION
Identifying the best multifocal IOL candidates begins with detailed preoperative assessment of each patient’s overall psychological and visual status. We have advanced technology that can deliver precise and accurate ocular measurements, but we must recognize the limitations of each technology. Proper awareness can lead to a reduction in our surgical error rate and optimization of our visual and refractive outcomes. Every cataract surgeon should respect the recommendation criteria for multifocal IOL implantation in order to provide long-term visual satisfaction for patients.

