


The popularity of toric IOLs has grown, with four FDA-approved lenses available on the US market. Precise alignment of these implants is critical to achieving good refractive outcomes. A common reason for misalignment is imprecise preoperative measurements,1 which can lead to inaccurate IOL positioning. Just 1º off of the desired axis can reduce cylinder power by up to 3.3%, and a 30º off-axis rotation can induce new astigmatism.2 The process of eliminating these errors of misalignment has evolved from conventional methods of marking reference points with an ink pen to digitally assisted methods involving smartphones to fully integrated, computerized digital systems and intraoperative aberrometry.
Precise toric IOL alignment depends on three basic steps: (1) determination of the steep axis, (2) marking of the steep axis, and (3) placement of the toric IOL at the desired axis. Other articles in this issue address the first and third steps; this one focuses on the marking of the steep axis with conventional marking tools, what the majority of surgeons are using today.
Categorically, steep axis marking can be grouped into orientation-based and landmark-based approaches. With the former, the steep axis is marked relative to a reference meridian—typically, the horizontal 0º and 180º axes. With landmark-based marking, the steep axis is referenced to an anatomical landmark on the iris, limbus, or cornea.
Conventional toric markers rely on orientation-based methods and typically require two steps. First, the reference axis is marked while the patient is in an upright position to minimize cyclotorsion in the supine position. Then, the steep axis is marked relative to the original reference, usually intraoperatively (although one-step markers combining both steps preoperatively are available).
CONVENTIONAL HANDHELD MARKERS
Marking the reference axis while the patient is upright can be accomplished using four different methods/tools: the slit-lamp beam, a tonometer-held marker, a bubble marker, or a pendulum marker:
• A narrow slit-lamp beam is typically turned to the 3- and 9-o’clock positions, allowing the limbus to be marked with either a small-gauge needle (micropuncture on the cornea) or an ink-marking pen.
• Similar markings can be made by replacing the Goldman tonomoter tip with an axis marker (ie, ToMark corneal marker [Geuder]; Figure 1).
• A bubble marker uses a bubble level to maintain the horizontal meridian in a handheld instrument (ie, Nuijts-Lane Pre-op Toric Reference Marker With Bubble [ASICO]; Figure 2).
• A pendular or weighted handheld marker allows gravity to level the instrument and place a reference point at the horizontal meridian (ie, Whitehouse Gravity Axis Marker [Rumex]; Figure 3).
With the reference mark placed preoperatively, an intraoperative device, such as the Mendez gauge, is then used to mark the desired steep axis, relative to the reference.
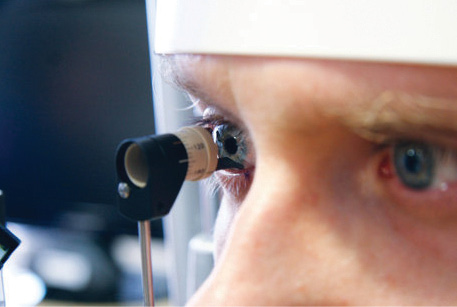
Figure 1. ToMark corneal marker placed on tonometer apparatus being used to make marks at the desired meridian.
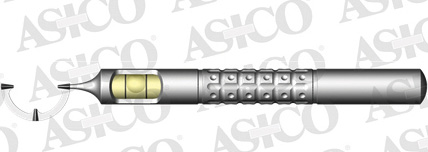
Figure 2. Nuijts-Lane bubble marker used to make reference marks at 0º, 90º, and 180º.

Figure 3. Whitehouse Gravity Axis Marker makes reference marks at 3, 6, and 9 o’clock with rear-positioned weight.
A comparative study of these four conventional methods showed the pendular marker to be slightly more accurate in terms of rotational misalignment than the others (mean 1.8º of rotation compared to 4.7º for tonometer marking).3 The tonometer-based method was found to be the least accurate with respect to axis marking. This was ascribed to the marker’s not touching/marking both sides of the limbus consistently.
DIGITAL-ASSIST MARKERS
A number of handheld digital devices have been developed to aid surgeons.
The Robomarker (Surgilum), a variant of a pendular marker, achieves one-step marking of the steep axis using pre-inked single-use tips, with a built-in fixation light. The AXsys (ASICO) is a digital variant of a bubble level marker that uses light-emitting diode lights and a pattern of audible beeps to confirm the horizontal meridian.
A few smartphone apps are available to assist conventional handheld markers. Axis Assistant is a variant of the slit lamp-based marker, where the steep axis can be marked preoperatively using the smartphone leveler. Similarly, toriCam uses the smartphone camera (and leveler) to photograph a surgeon’s reference marks and measure the actual achieved axis to within 1º.
At a Glance
• The precise aligment of toric IOLs is critical to achieving good outcomes.
• Steep axis marking can be categorized into either landmark-based or orientation-based approaches.
• Four different tools are used for marking the axis when the patient is upright: the slit-lamp beam, a tonometer-held marker, a bubble marker, or a pendulum marker.
The accuracy of all these orientation-based methods depends on factors that are difficult to control such as the skill of the user, the subjective avoidance of head tilt on the part of the patient, and the bleeding of even fine-tipped ink-based markers. (Thermadot cautery attempts to address this for intraoperative marking but does not help with reference marking.)
Landmark-based, automated and integrated digital overlay systems (discussed elsewhere in this issue) are likely to decrease the rotational axial error compared with current conventional markers but at a substantial cost. Studies comparing the two methods are ongoing.
SUMMARY
Proper alignment is key to success with toric IOLs, and numerous tools are available to help surgeons accurately mark the steep axis. For many ophthalmologists, conventional marking tools are a cost-effective and accurate method for toric IOL markings. Even with the advent of integrated digital overlay systems and intraoperative aberrometry, a preplaced mark can serve as an accurate backup in toric IOL cases. n
1. Hirnschall N, Hoffmann PC, Draschl P, et al. Evaluation of factors influencing the remaining astigmatism after toric intraocular lens implantation. J Refract Surg. 2014;30(6):394-400.
2. Cha D, Kang S, Kim S, et al. New axis-marking method for a toric intraocular lens: mapping method. J Refract Surg. 2011;27(5):375-379.
3. Popp N, Hirnschall N, Maedel S, Findl O. Evaluation of 4 corneal astigmatic marking methods. J Cataract Refract Surg. 2012;38(12):2094-2099.
Kunal Merchant, MD
• Department of Internal Medicine, Lankenau Medical Center, Wynnewood, Pennsylvania
• ophthalmology resident, George Washington University, Washington, DC
• merchant.kunal5@gmail.com
• Financial disclosure: None acknowledged
Tal Raviv, MD
• founder and medical director, Eye Center of New York
• clinical associate professor of ophthalmology, New York Eye and Ear Infirmary of Mount Sinai
• (212) 889-3550; talraviv@eyecenterofny.com; Twitter @TalRavivMD
• Financial disclosure: None acknowledged

