Case 1
Details
- - A 61-year-old woman
- - Minor dry eye symptoms, most prominent in the morning
- - Desires an extended depth of focus IOL
Thanks for visiting CRSToday. Our advertisers are important supporters of this site, and content cannot be accessed if ad-blocking software is activated.
In order to avoid adverse performance issues with this site, please white list https://crstoday.com in your ad blocker then refresh this page.
Need help? Click here for instructions.
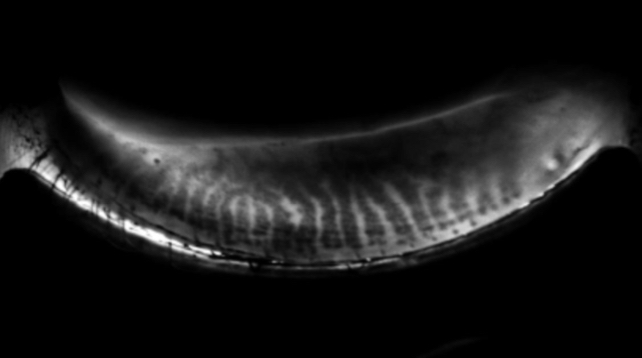
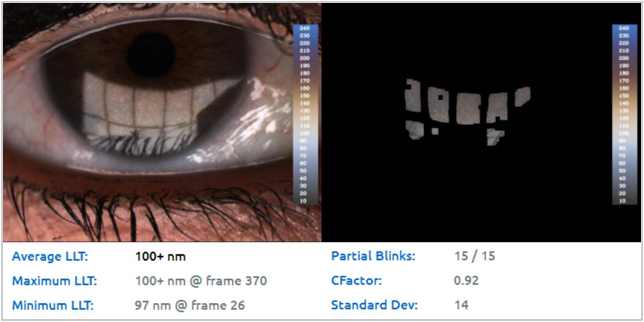
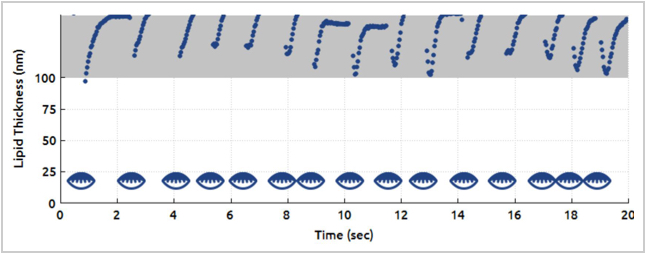
A 61-year-old woman who was a previously practicing optometrist presented for cataract surgery and expressed interest in a TECNIS SYMFONY IOL.* Casey Claypool, OD, at Empire Eye Physicians examined her 1 month prior and noted an overall 2+ meibomian gland dysfunction (MGD) characterized by 1+ telangiectasis of the lid margins, poor expressibility of the meibum, and 2+ turbidity of the meibum. An incomplete blink and an average lipid layer thickness of 100 nm was noted on LIPIVIEW II* reports. Dynamic Meibomian Imaging demonstrated minimal gland loss, with mild truncation, but overall decent meibomian gland architecture. At this time, she reported minor dry eye symptoms, including visual fluctuations and a significant increase in symptoms in the morning that persisted until she instilled artificial tears. Treatment with vectored thermal pulsation therapy was performed. After the LIPIFLOW* treatment, the patient noted a reduced reliance on artificial tears and that her morning dry eye symptoms were much improved. Seven weeks later, she presented to me for cataract surgery and preoperative testing showed a 1.00 D shift in IOL recommendation compared with biometry measurements taken 3 months prior. Ultimately, a +22.50 D TECNIS SYMFONY* was selected. At 1 day postoperative, the patient's VA was 20/20 at both distance and near and 20/16 at intermediate range.

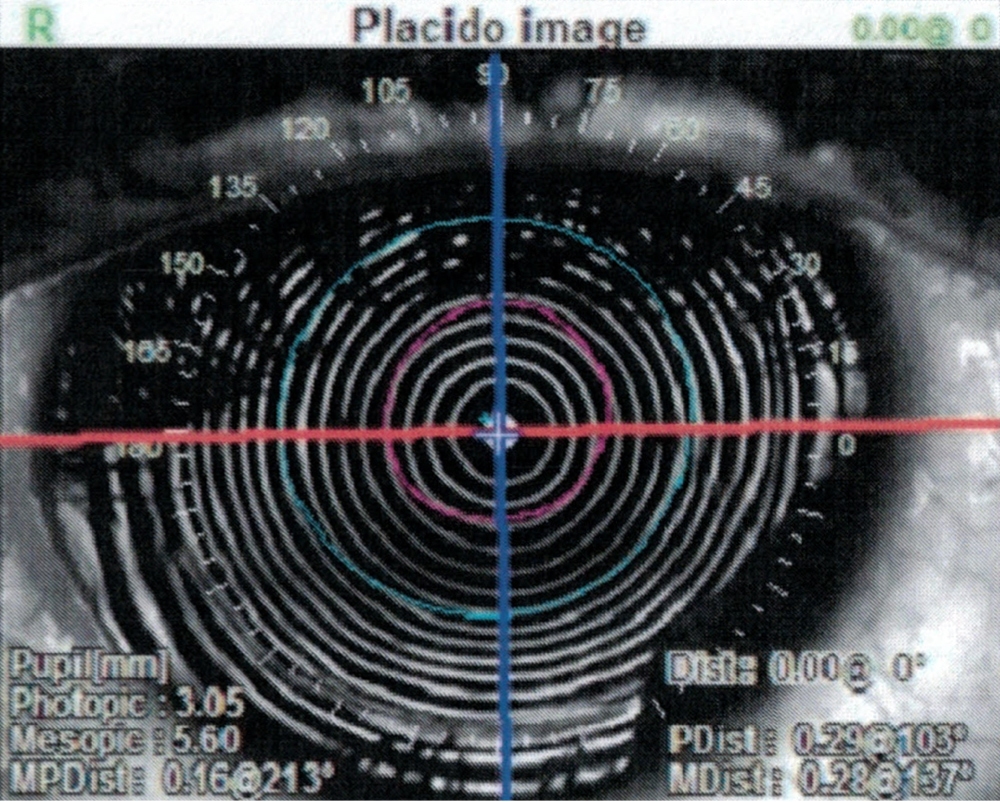
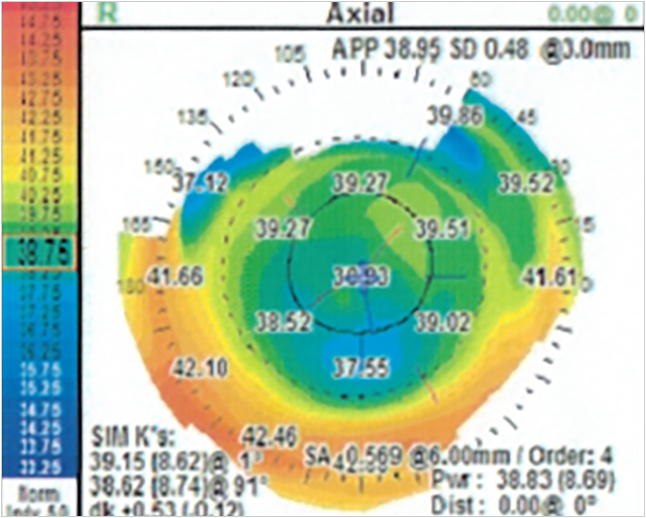
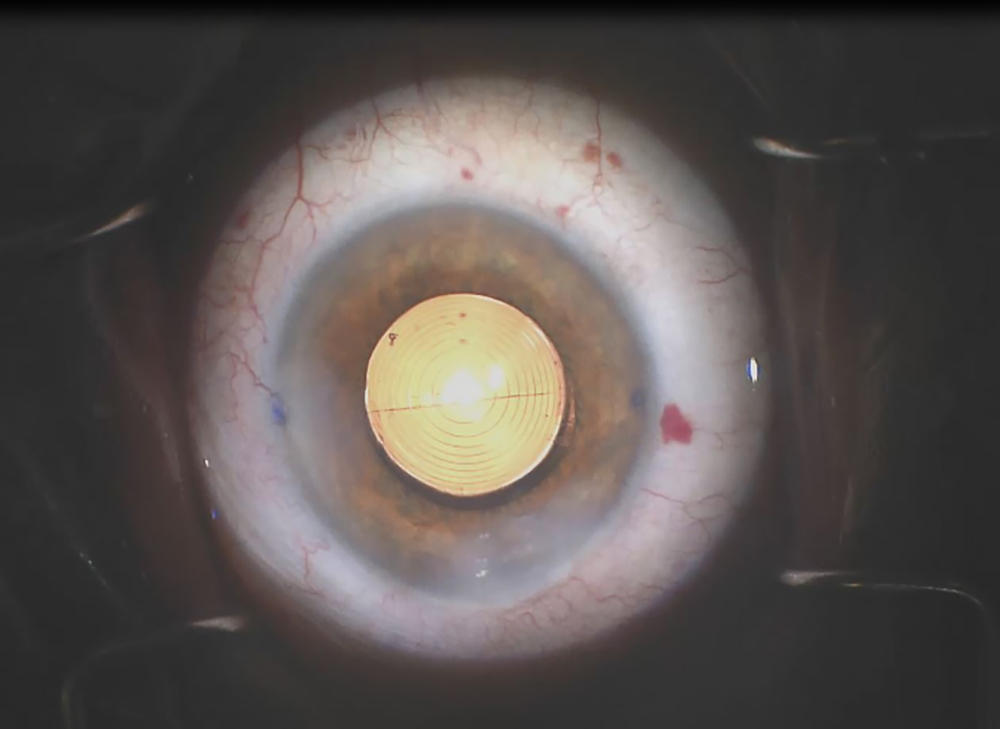
A 33-year-old male accountant presented for a LASIK consultation with symptoms of itching, burning, and tearing with fluctuations in vision depending on the time of day. In the past 10 years, contact lens intolerance prevented him from wearing contact lenses while at work given his extended use of computers during the day, and glasses proved cumbersome and limiting during recreational activities. This patient had sought laser vision correction in the past at several other practices and was deemed a “non-candidate” because of his dry eyes. His symptoms had not improved significantly with preservative-free artificial tears, immunomodulators, punctal occlusion, or a previous trial of amniotic membrane.
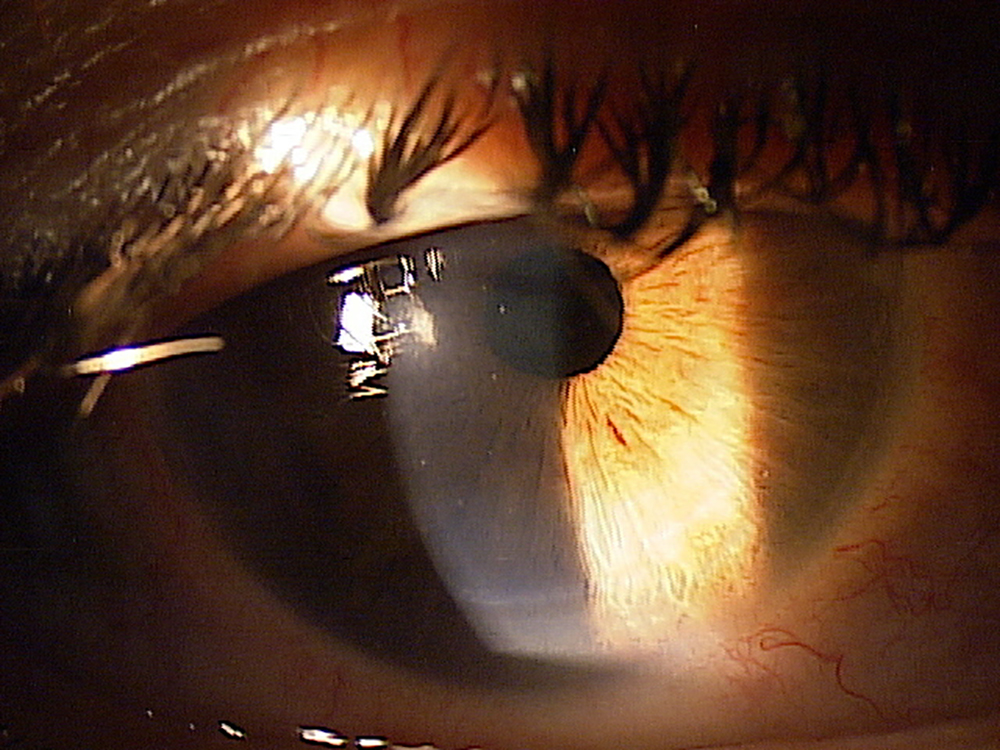
Examination of the lid margins showed meibomian gland inspissation, mild telangiectasia, and capped glands. Meibomian gland expression revealed turbidity in the meibum. Lid eversion showed mild bilateral upper and lower lid papillary reaction. Slit-lamp examination showed conjunctival perilimbal staining, dense superficial punctate keratitis and mild conjunctival erythema. Early evidence of gland atrophy was noted on LIPISCAN images while HD Analyzer showed high Ocular Scatter Index Scores, 1.58 ± 0.52 with evidence of an unhealthy tear film and quick breakup time. The patient elected vectored thermal pulsation therapy and noted an increase in tear production and a decrease in light sensitivity, as well as an increase in duration of comfortable contact lens wear time. Examination revealed a marked decrease in conjunctival and corneal staining and improvement in gland fuction. A repeat HD Analyzer was performed with a reduction in OSI, 0.74 ± 0.07, as well as a stable, flat tear film. After 3 months of being relatively symptom free, the patient elected to undergo laser vision correction. On day 1 postop his visual acuity was 20/15 OU and there was no evidence of SPK noted at week 1 postop. One year after the surgery and LIPIFLOW treatment this patient is 20/15 with no recurrence of dry eye signs and symptoms. Repeat LIPISCAN showed no evidence of further meibomian gland atrophy.

Week 1
IOL Recommendation: +23.50 D
Mean OSI: 1.58 ± 0.52 OSI Evolution With Time
3 days later
Weeks 1-6
To supplement his treatment, he was prescribed Lotemax gel .05% (Bausch + Lomb) bid for one week, along with Omega 3 supplementation.
Week 6
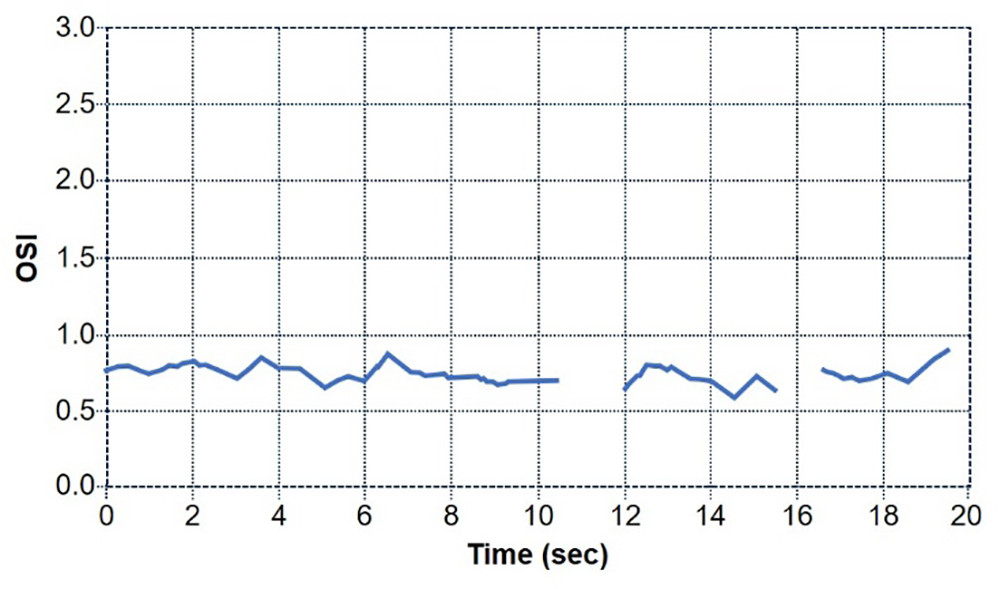
Mean OSI: 0.74 ± 0.07 OSI Evolution With Time
Weeks 6-19
Patient was able to comfortably wear contact lensese for an extended amount of time.
A 33-year-old male accountant presented for a LASIK consultation with symptoms of itching, burning, and tearing with fluctuations in vision depending on the time of day. In the past 10 years, contact lens intolerance prevented him from wearing contact lenses while at work given his extended use of computers during the day, and glasses proved cumbersome and limiting during recreational activities. This patient had sought laser vision correction in the past at several other practices and was deemed a “non-candidate” because of his dry eyes. His symptoms had not improved significantly with preservative-free artificial tears, immunomodulators, punctal occlusion, or a previous trial of amniotic membrane.
Examination of the lid margins showed meibomian gland inspissation, mild telangiectasia, and capped glands. Meibomian gland expression revealed turbidity in the meibum. Lid eversion showed mild bilateral upper and lower lid papillary reaction. Slit-lamp examination showed conjunctival perilimbal staining, dense superficial punctate keratitis and mild conjunctival erythema. Early evidence of gland atrophy was noted on LIPISCAN images while HD Analyzer showed high Ocular Scatter Index Scores, 1.58 ± 0.52 with evidence of an unhealthy tear film and quick breakup time. The patient elected vectored thermal pulsation therapy and noted an increase in tear production and a decrease in light sensitivity, as well as an increase in duration of comfortable contact lens wear time. Examination revealed a marked decrease in conjunctival and corneal staining and improvement in gland fuction. A repeat HD Analyzer was performed with a reduction in OSI, 0.74 ± 0.07, as well as a stable, flat tear film. After 3 months of being relatively symptom free, the patient elected to undergo laser vision correction. On day 1 postop his visual acuity was 20/15 OU and there was no evidence of SPK noted at week 1 postop. One year after the surgery and LIPIFLOW treatment this patient is 20/15 with no recurrence of dry eye signs and symptoms. Repeat LIPISCAN showed no evidence of further meibomian gland atrophy.
Week 1
Mean OSI: 1.58 ± 0.52 OSI Evolution With Time
3 days later
Weeks 1-6
To supplement his treatment, he was prescribed Lotemax gel .05% (Bausch + Lomb) bid for one week, along with Omega 3 supplementation.
Week 6
Mean OSI: 0.74 ± 0.07 OSI Evolution With Time
Weeks 6-19
Patient was able to comfortably wear contact lensese for an extended amount of time.
Month 16
The patient in this case is employed by Johnson & Johnson Vision.
PP2019TS4278
The LipiFlow® Thermal Pulsation System is intended for the application of localized heat and pressure therapy in adult patients with chronic cystic conditions of the eyelids, including meibomian gland dysfunction (MGD), also known as evaporative dry eye or lipid deficiency dry eye.
Do not use the LipiFlow® System in patients with the following conditions. Use of the device in patients with these conditions may cause injury. Safety and effectiveness of the device have not been studied in patients with these conditions.
The Activator or Activator II (Disposable) may not fit all eyes, such as eyes with small palpebral fornices
Use of the LipiFlow® System in patients with the following conditions may result in reduced treatment effectiveness because these conditions may cause ocular symptoms unrelated to cystic meibomian glands and require other medical management. Safety and effectiveness of the device have not been studied in patients with these conditions.
In addition, the treatment procedure may loosen previously inserted punctal plugs, which may worsen the patient’s dry eye symptoms.
Potential adverse effects that may occur as a result of the procedure include, but are not limited to, the onset or increase in:
Potential serious adverse events (defined as permanent impairment or damage to a body structure or function or necessitates medical or surgical intervention to preclude permanent impairment or damage to a body structure or function) that are not anticipated because of the device mitigations to prevent occurrence include:
Reference the LipiFlow Thermal Pulsation System Instructions for Use for a complete listing of indications, warnings, and precautions.
The LipiView II Ocular Surface Interferometer is an ophthalmic imaging device that is intended for use by a physician in adult patients to capture, archive, manipulate and store digital images of:
Contraindications are conditions in which the device should not be used because the risk of use clearly outweighs any benefit. No contraindications have been identified for LipiView II.
The following patient conditions may affect the interferometry assessment of a patient’s tear film using LipiView II:
There are no known or anticipated adverse effects associated with use of this device.
Reference the LipiView II Ocular Surface Interferometer Instructions for Use for a complete listing of indications, warnings, and precautions.
LipiScan™ Dynamic Meibomian Imager (DMI) is an ophthalmic imaging device intended for use by a physician in adult patients to capture, archive, manipulate and store digital images of the meibomian glands.
No contraindications have been identified for the LipiScan™.
Caution: Disinfect the surfaces of the chin rest, forehead rest and Handheld Near Infrared (IR) Lid Everter with isopropyl alcohol immediately prior to use and prior to storage to prevent cross-contamination and patient infection.
There are no known or anticipated adverse effects associated with use of this device.
Reference the LipiScan Dynamic Meibomian Imager Instructions for Use for a complete listing of indications, warnings, and precautions.
The Meibomian Gland Evaluator is a hand held instrument used by a physician to evaluate Meibomian gland secretions in adult patients during a routine eye examination. The instrument provides a standardized method to apply consistent, gentle pressure to the outer skin of the lower eyelid while visualizing the secretions from the Meibomian gland orifices through a slit lamp biomicroscope.
No contraindications are known.
Potential adverse effects that are unlikely but may occur with use of the Meibomian Gland Evaluator include but are not limited to:
Reference the Meibomian Gland Evaluator Package Insert for a complete listing of indications, warnings, and precautions.
The TECNIS Symfony Extended Range of Vision IOL, Model ZXR00, is indicated for primary implantation for the visual correction of aphakia, in adult patients with less than 1 diopter of pre-existing corneal astigmatism, in whom a cataractous lens has been removed. The lens mitigates the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, the lens provides improved intermediate and near visual acuity, while maintaining comparable distance visual acuity. The Model ZXR00 IOL is intended for capsular bag placement only.
Patients with any of the conditions described in the Directions for Use may not be suitable candidates for an intraocular lens because the lens may exacerbate an existing condition, may interfere with diagnosis or treatment of a condition, or may pose an unreasonable risk to the patient’s eyesight. Lenses should not be placed in the ciliary sulcus. May cause a reduction in contrast sensitivity under certain conditions, compared to an aspheric monofocal IOL; fully inform the patient of this risk before implanting the lens. Special consideration should be made in patients with macular disease, amblyopia, corneal irregularities, or other ocular disease. Inform patients to exercise special caution when driving at night or in poor visibility conditions. Some visual effects may be expected due to the lens design, including: a perception of halos, glare, or starbursts around lights under nighttime conditions. These will be bothersome or very bothersome in some people, particularly in low-illumination conditions, and on rare occasions, may be significant enough that the patient may request removal of the IOL.
Interpret results with caution when refracting using autorefractors or wavefront aberrometers that utilize infrared light, or when performing a duochrome test. Confirmation of refraction with maximum plus manifest refraction technique is recommended. The ability to perform some eye treatments (e.g. retinal photocoagulation) may be affected by the optical design. Target emmetropia for optimum visual performance. Care should be taken to achieve IOL centration, as lens decentration may result in a patient experiencing visual disturbances under certain lighting conditions.
The most frequently reported serious adverse events that occurred during the clinical trial of the TECNIS Symfony lens were cystoid macular edema (2 eyes, 0.7%) and surgical reintervention (treatment injections for cystoid macular edema and endophthalmitis, 2 eyes, 0.7%). No lens-related adverse events occurred during the trial.
Reference the Directions for Use for a complete listing of Indications and Important Safety Information
© 2026 Bryn Mawr Communications, LLC. All Rights Reserved | Privacy Policy