
Presbyopia-correcting intraocular lenses (PCIOLs) are an advanced technology for cataract surgery that have been reported to reduce the dependence on spectacles and provide a wider range of vision than monofocal intraocular lenses (IOLs).1
Trifocal IOLs and extended depth of focus IOLs, such as the PanOptix® and Vivity® IOLs, respectively, are PCIOLs that build on the visual quantity and quality of multifocal IOLs from the early 2000s.2;3
Light-adjustable lenses (LALs) are the first IOLs to allow adjustment after cataract surgery and represent another recent entrant to the cataract refractive space.4;5
Previous works have discussed factors that influence the choice of IOL for patients,6;7 such as visual outcomes, likelihood of side effects or preference for spectacle independence,7 but there is less information available on the workflow implications associated with offering these recent entrants, such as resource use required.
LALs require additional resources and visits in the post-operative period to obtain patient satisfaction with visual outcomes and optimal refraction post-surgery,8 and there has been no published work on the pre-operative resource requirements for LALs.
One study using patients from 2019 and prior has reported that additional post-operative time is required for PCIOLs compared to monofocal IOLs,9 but there have been no more recent publications on the post-operative period or any on the pre-operative or intra-operative period.
This survey aimed to understand the resource requirements, implementation success pertaining to pre-, intra-, and post-operative logistics, and general patient satisfaction associated with latest-generation IOL types (PCIOLs or LALs) for ophthalmologists and their practices.10
Collecting surgeon experiences with the implementation of PCIOLs and LALs
Forty ophthalmic surgeons from the United States, experienced in implanting PCIOLs and LALs, were recruited to participate in a 38-question survey. The survey aimed to understand their experiences with the time and resources required to care for patients with PCIOLs or LALs, as well as their perceptions of patient satisfaction with these technologies (Table 1). Resident surgeons, retired surgeons, and surgeons who did not have experience implanting both PCIOLs and LALs were excluded from this survey.10

Table 1: Topics of Information Collected by Survey
Respondents came from a variety of practice types, including ambulatory surgical center (ASC)/private practice with ASC attachment (n=11), solo practices (n=9), large, multi-specialty/multi-surgeon practice (n=9), smaller, private/group practice (n=9), and teaching facilities (n=2).
Surgeons also reported a variety of practice staff, including ophthalmologists, optometrists, technicians, nurses, and administrative staff. Surgeons reported a mean annual cataract surgery volume of 785 procedures per year, with a range of 100 to 2,500 surgeries per year.
Resource Requirements for LALs
Pre-operative and Intra-operative Period
Surveyed surgeons reported a mean length of 24 minutes required for pre-operative LAL patient consultation.
Forty-five percent of surgeons reported the time required for pre-operative consultation with LALs was more or much more than expected.
When asked if the steps involved for LAL pre-operative work-up were more or less than expected, 22.5% of surgeons indicated the steps for LALs were more or much more than they expected.
Surgeons were asked whether surgical procedures with LALs took longer than a standard monofocal IOL, and 65% responded ‘no’.
Post-operative Period
Surveyed surgeons reported an average number of 5.3 LAL follow-up appointments (range 2 to 10).
Fifty-five percent of surveyed surgeons reported that the length of time for an average follow-up appointment was “more” or “much more” than expected.
Similarly, more than half of surveyed surgeons reported that the number of average follow-up appointments was “more” or “much more” than expected (Figure 1).

Figure 1: Proportion of surgeons reporting on expectations of number and length of LAL followup appointments
When asked about the proportion of patients who require additional intervention (defined as IOL rotation, LASIK touch up or extended LDD treatment) to ensure satisfaction, 17.5% of surgeons reported the number was more than expected for LAL recipients.
Forty percent of surgeons reported that patients obtain satisfactory visual outcomes within one month for LAL implantation.
Conclusions
Overall, the majority of respondents reported that the resources required to prepare and care for LAL recipients in the post-operative periods were generally more time consuming than expected, while a smaller proportion of surgeons reported that pre-operative consultation and work-up steps for LAL were more time consuming than expected.
There is currently a lack of published evidence on the resource requirements for LALs. Nishihara et al. (2023) conducted a cost-effectiveness analysis comparing LALs and monofocal IOLs, and found that LALs had higher costs due to capital acquisition costs and the additional post-operative appointments, the impact of which may be underestimated given the analysis did not factor in the additional staff/facility costs associated with the extra time required for each pre- and post-operative appointment.11
These findings may help eye care providers better plan the resources required to successfully implement LAL into their practice workflow.
Resource Requirements for PCIOLs
Pre-operative and Intra-operative Period
Surveyed surgeons reported a mean length of 17 minutes for a pre-operative PCIOL patient consultation.
7.5% of surgeons reported the time required for pre-operative consultation with PCIOLs was more or much more than expected.
When asked if the steps involved for PCIOL pre-operative work-up were more or less than expected, 2.5% of surgeons indicated the steps for PCIOL were more or much more than they expected.
Surgeons were asked whether surgical procedures with PCIOLs took longer than a standard monofocal IOL, and 85% responded ‘no’.
Post-operative Period
Surveyed surgeons reported an average of 2.8 PCIOL post-operative appointments, with a range of between 2 to 4 appointments reported.
When asked about the number of follow-up appointments, 2.5% of surveyed surgeons reported that the number of follow-up appointments was “more” or “much more” than expected.
All surgeons reported that the length of time for an average follow-up appointment was “as expected”, “less than expected“, or “much less than expected” (Figure 2).
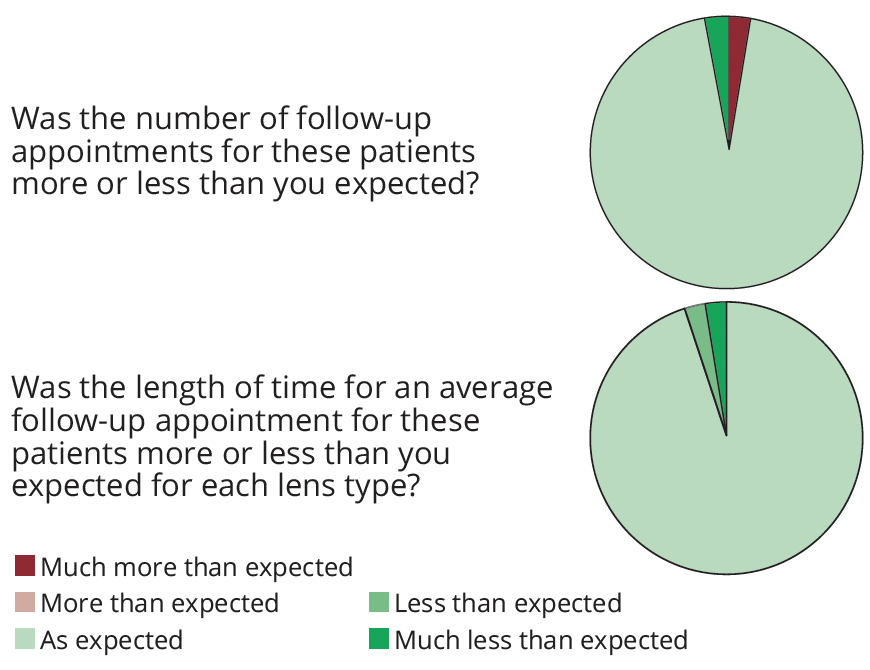
Figure 2: Proportion of surgeons reporting on expectations of number and length of PCIOL follow-up appointments
When asked about the proportion of patients who require additional intervention to ensure satisfaction, all surgeons reported the number was “as expected”, “less than expected“, or “much less than expected” for PCIOL recipients.
Eighty-seven percent of surgeons reported that patients obtain satisfactory visual outcomes within a month of PCIOL implantation.
The majority of surgeons reported that the pre-operative and post-operative time requirements took the expected length of time for PCIOL patients, and 85% reported that PCIOLs did not take longer during the cataract surgical procedures than a standard monofocal IOL.
Previous work by Maloney et al. (2023) found that PCIOL recipients generally require more post-operative care than monofocal IOL recipients,
with a higher number of visits, longer mean visit duration and more post-operative procedures.9
Although PCIOLs may take more time than monofocal IOLs, surgeons generally report that the amount of appointments and time required is in line with their current expectations for these IOLs.
Ophthalmologists may use these findings to optimize clinic workflows associated with PCIOL delivery and management and support more efficient patient through-put.
Discussion
Given the limited data on PCIOLs and LALs in the context of clinic workflow, this study could help eye care providers make a more informed decision regarding the adoption or recommendation of these technologies or planning resources for their clinic.
There are several strengths associated with this survey, including methodological advantages which reduce bias and encourage honest reporting from respondents (recruitment by an independent research organization, anonymous reporting), and the diversity of respondents, representing a range of practice settings.
Furthermore, the study assessed resource requirements across the entire patient journey and was not limited to post-operative care.
Finally, the sample size exceeds that reported in similar surveys published in ophthalmology.12;13
This study shares several limitations common to all survey-based research, including subjective responses and the possibility of recall bias. However, this limitation was likely mitigated due to the criteria that all surgeons were working with both devices at the time of enrollment.
Future studies should consider using alternative methodologies that allow objective and quantitative comparison of differences in the work intensity and resource use between PCIOLs and LALs.
1. Sun Y, Hong Y, Rong X, Ji Y (2022) Presbyopia-correcting intraocular lenses implantation in eyes after corneal refractive laser surgery: a meta-analysis and systematic review. Frontiers in Medicine 9 834805.
2. Cho J-Y, Won YK, Park J, Nam JH, Hong J-Y et al. (2022) Visual outcomes and optical quality of accommodative, multifocal, extended depth-of-focus, and monofocal intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and bayesian network meta-analysis. JAMA Ophthalmology 140 (11): 1045-1053.
3. Hovanesian JA, Jones M, Allen Q (2022) The vivity extended range of vision IOL vs the PanOptix trifocal, ReStor 2.5 active focus and ReStor 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle independence. Clinical Ophthalmology 145-152.
4. RxSight (Web Page) Light Adjustable Lens™. Updated Available online at: https://rxsight.com/healthcare-professionals/. Accessed: August 15 2024.
5. U.S. Food and Drug Administration (Web Page) FDA approves first implanted lens that can be adjusted after cataract surgery to improve vision without eyeglasses in some patients. Updated November 22, 2017. Available online at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-implanted-lens-can-be-adjusted-after-cataract-surgery-improve-vision-without. Accessed: August 15 2024.
6. Lapp T, Wacker K, Heinz C, Maier P, Eberwein P et al. (2023) Cataract surgery—indications, techniques, and intraocular lens selection. Deutsches Ärzteblatt International 120 (21-22): 377.
7. Kabbani J, Price L, Patel R, Din N, Bizrah M (2024) A survey of intraocular lens preferences of UK refractive surgeons for cataract surgery and refractive lens exchange. BMC Ophthalmology 24 (1): 397.
8. RxSight (11/22/2017) Light Adjustable Lens (LAL) and Light Delivery Device (LDD) for the Correction of Aphakia and Reduction of Residual Astigmatism: Professional Use Information. In. Food Drug and Administration.
9. Maloney RK, Doane J, Weinstock R, Donaldson KE (2023) Work Intensity of Postoperative Care Following Implantation of Presbyopia-Correcting versus Monofocal Intraocular Lenses. Clinical Ophthalmology 17 1993-2001.
10. Alcon Data on File, 2024. REF-22724.
11. Nishihara TW, Hu JQ, Buchholz RD, Murphy JD, Afshari NA (2023) Cost-Effectiveness Analysis of Light Adjustable Lens Compared to Monofocal Intraocular Lens in Cataract Surgery. Journal of Refractive Surgery 39 (11): 777-782.
12. Yim CK, Teng CC, Warren JL, Tsai JC, Chadha N (2020) Microinvasive glaucoma surgical training in United States ophthalmology residency programs. Clinical Ophthalmology 14 1785-1789.
13. Ifantides C, SooHoo JR, Christopher KL (2023) Impact of a formal manual small-incision cataract surgery curriculum in an American ophthalmology residency program. Indian Journal of Ophthalmology 71 (6): 2474-2477.
Abbreviations: ASC = Ambulatory surgical center; IOL = intraocular lens; LAL = light adjustable lens; PCIOL = presbyopia-correcting IOL.
The views and opinions expressed here may not necessarily represent those of Bryn Mawr Communications or Cataract & Refractive Surgery Today.
© 2025 Alcon Inc. US-ACP-2400012


