
Darrell White, MD: We have convened this panel of ophthalmologists and optometrists to share our viewpoints about the state of dry eye disease (DED) and, specifically, how a topical formulation, CEQUA (cyclosporine ophthalmic solution) 0.09% (Sun Ophthalmics) fits into our varied practices. In this roundtable, we will discuss the challenges of patient discontinuation and the clinical need for a topical DED therapy that is comfortable, tolerable, and efficacious for patients.
THE PREVALENT PROBLEM OF DED
Dr. White: Whenever we talk about DED, it’s important to define it. DED is a multifactorial, immune-mediated inflammatory disorder of the ocular surface.1,2 It is characterized by a loss of tear film homeostasis, which ignites inflammatory cytokines that interrupt the natural feedback loop between the ocular surface, specifically the lacrimal functional unit, the lacrimal glands, goblet cells, meibomian glands, and the brainstem.1-5 A negative feedback loop begins: inflammation begets dryness, which begets inflammation, which begets dryness, and this cycle progressively worsens.
The three mainstay pharmaceutical options to treat this DED cycle include CEQUA (cyclosporine ophthalmic solution) 0.09%, Restasis® (cyclosporine ophthalmic emulsion) 0.05% (AbbVie/Allergan, Inc.), and Xiidra® (lifitegrast ophthalmic solution) 5% (Bausch + Lomb).1 These are all anti-inflammatory agents, all indicated for the long-term treatment of DED, and they are also immunomodulators that work differently from ocular steroids and the older anti-inflammatories.
THE CHALLENGE OF PATIENT ADHERENCE TO DED MEDICATION
Dr. White: The entirety of the DED pharmaceuticals market suffers from low patient adherence. There are high rates of discontinuation of dry eye therapies in general, but specifically with immunomodulators. In a study that colleagues and I conducted in 2019, we showed that the majority of patients who were on Restasis and Xiidra discontinued the treatments within 12 months.6
Having used these medications in our practices, we can all attest that they can cause burning and stinging upon instillation.7 Additionally, there can be significant lag time between patients’ initiating treatment and when they experience symptomatic relief.6 Yet, when patients discontinue their treatments, DED can progress and become more complex.
Dr. Johnston, what’s been your experience with patients discontinuing treatment with immunomodulators?
Dr. Johnston: I see a wide spectrum of patients who discontinue prescription DED drops because they don’t experience enough symptomatic improvement, can’t tolerate the side effects, or a combination of the two. We needed something that could overcome these challenges to improve DED drop compliance.
Dr. White: Dr. Parekh, how long are DED patients usually willing to go without having a breakthrough?
Dr. Parekh: It depends on how the patient presents to your practice. Those who have been kicked around in the healthcare system with untreated DED want to get better yesterday, but are frustrated. Most people want improvement within several weeks to 1 or maybe 2 months. Four to 6 months is too late; you’ve probably “lost” the patient. It’s very important for us to start our patients on the path to a healthier cornea as soon as possible.
THE FORMULATION OF CEQUA
Dr. White: Dr. Johnston, what role can a product’s formulation play in its tolerability and helping patients stay on therapy?
Dr. Johnston: Cyclosporine is a familiar molecule, and it has enjoyed a large market share because, overall, it’s efficacious. However, there is room for a topical therapy that is potent, has increased bioavailability, and ultimately works in as little as 2 weeks to improve patients’ symptoms. I think Sun Ophthalmics has delivered on those goals by developing a novel platform for cyclosporine—a re-engineering of a familiar treatment option.
An eye drop’s inactive ingredients can have a significant effect on its safety and efficacy. CEQUA is a clear, nonpreserved drop that is isotonic, meaning it has a neutral pH in a vehicle that provides comfort and minimizes adverse reactions.
When I first got access to CEQUA and put it in my eye, I was encouraged that I didn’t experience dysgeusia, visual blurring, or significant burning. Dr. White, what was your first impression when you tried CEQUA? Did you find it comfortable and easy to tolerate?
Dr. White: You may not know this, Dr. Johnston, but I have had bitterly symptomatic DED since I was in my mid-twenties. I try every single dry eye medication on the market. When CEQUA was first available, I put it right in my eye, and it was just a really comfortable application. I had a sense of relief when it went in. I think my comfort was, in part, due to the CEQUA vehicle, as you described.
Dr. Johnston: Great points, Dr. White. Again, the researchers at Sun Ophthalmics wanted to create a novel delivery platform to improve the bioavailability and action time of cyclosporine. They achieved that goal by applying the novel NCELL® Technology, which uses nanomicelles to deliver cyclosporine A to the ocular tissues (Figure 1).8-11

Figure 1. Unique NCELL technology used in CEQUA delivers more cyclosporine A to ocular tissues. NCELL technology used in CEQUA encapsulates cyclosporine in spheres, with a hydrophobic core and hydrophilic outer layer. These nanomicelles penetrate the aqueous layer of the tear film, thereby delivering cyclosporine directly to ocular tissues.8-12
They also improved cyclosporine’s solubility by engineering it to be encased in a hydrophilic outer shell. With this hydrophilic casing, the active cyclosporine molecule can penetrate the aqueous layer to release the nanomicellar cyclosporine particles upon the ocular surface.12 Therefore, this formulation increases the amount of medication delivered to the target tissues.
The data that really caught my attention were from the comparison study researchers conducted between commercially available 0.05% cyclosporine (Restasis) and cyclosporine 0.05% with the NCELL technology on 112 New Zealand white female rabbits. The rabbits were randomized to receive either commercially available Restasis or cyclosporine 0.05% with NCELL daily for 7 days.13 It’s worth noting that, whereas the CEQUA formulation available now is a 0.09% solution, in this study, it was tested at a strength of 0.05%—a truly apples-to-apples comparison with the Restasis formulation. The eyes that received cyclosporine 0.05% with NCELL showed up to three times the amount of absorption across ocular tissues in the eyes treated with Restasis.
safety & TOLERABILITY
Dr White: Let’s talk about the CEQUA safety profile. In its clinical trials, the most common adverse reactions reported in greater than 5% of subjects were instillation site pain (22%) and conjunctival hyperemia (6%). We should also advise patients that, to avoid the potential for eye injury and contamination, they should not touch the tip of the vial to the eye or other surfaces.
What are the most common adverse reactions you have seen in your clinical practice, and what has been your experience with patients’ tolerability of CEQUA?
Dr. Johnston: For any topical drop to succeed with patients, it must be well tolerated. Drop discomfort and pain leads to poor compliance and often the discontinuation of therapy.6 In its phase 2/3 clinical trial, most patients found CEQUA to be comfortable right from the start: 95% of the patients reported either no or mild instillation site pain.14 Additionally, no patient in the CEQUA clinical trial complained of dysgeusia or visual blurring. In fact, the package insert for CEQUA states that there are “no contraindications.”15 For this medication category, there is no other ocular medication that I know of that has no contraindications at all in its package insert. Based on these outcomes, I have no reservations about prescribing CEQUA in my practice.
Dr. White: Let’s pause briefly and take a poll. Is this the kind of tolerability we’re seeing in our clinics? Dr. Ayres, are you getting this kind of data in patients using CEQUA?
Dr. Ayres: Absolutely. I’ve been really impressed with the tolerability of cyclosporine in the form of CEQUA, and I think its nanomicellar technology is the key difference. Otherwise, it’s just cyclosporine. If a medication can’t reach its target tissue in a tolerable way, it doesn’t make a difference. When I first looked at these data, I thought, “Okay, we’ve got cyclosporine 0.9%, I also have it in 0.5%. Is it that big of a difference?” But it is. And the NCELL technology is what makes the difference to me.
Dr. Devries: I’ve found that the data reported in the study really is emulated in the clinical environment.
FAST IMPROVEMENT: 2-WEEK DATA FROM THE CLINICAL TRIAL
Dr. White: Dr. Parekh, besides the tolerability of CEQUA, we discussed that a slow speed of onset also contributes to patients discontinuing therapy. What have you seen in your practice?
Dr. Parekh: Within the landscape of DED, historically, available medications just haven’t worked quickly enough to keep patients compliant. To me, the clinical trial data for CEQUA on total corneal staining are incredibly important—the drop provides results in as little as 2 weeks (Figure 2).16,17 In the data I’m referring to, CEQUA was compared to its vehicle in a phase 2b/3, randomized, multicenter, double-masked, vehicle-controlled study. The conjunctival and corneal staining were assessed at baseline and on days 14, 28, 42, 56, and 84. After just 2 weeks, you start seeing the effect. These data are incredibly important to me, not only for my medical patients, but also for my surgical patients. We know that if surgical patients have ocular surface issues and dry eye, we have to improve their corneal staining as best we can preoperatively. This will yield the best surgical outcomes for our patients.
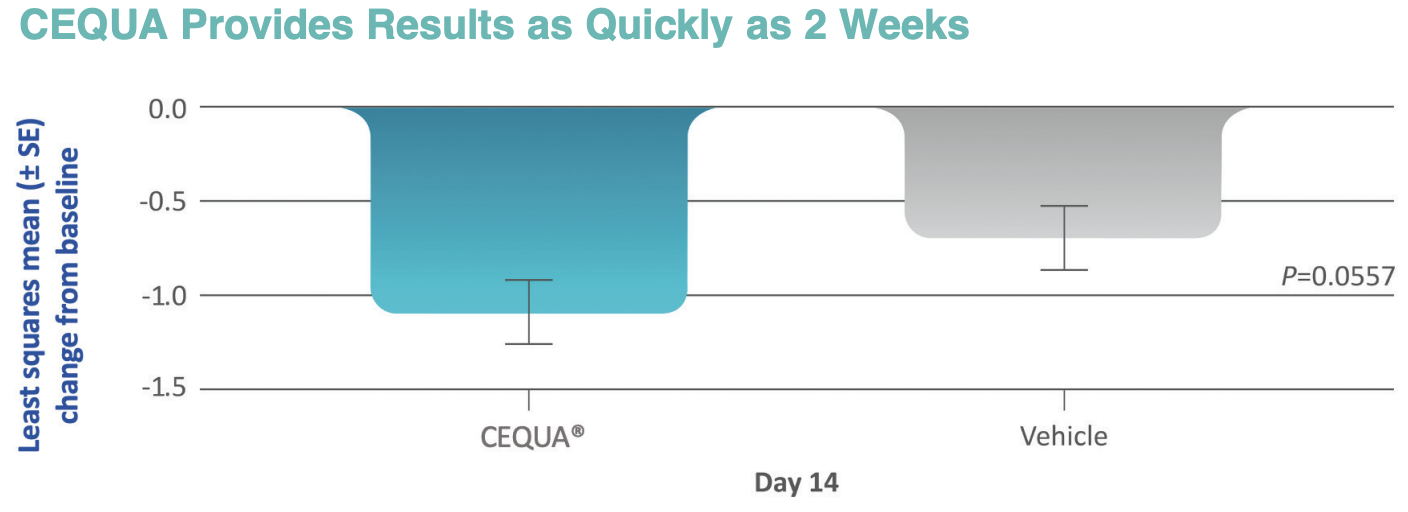
Figure 2. In clinical trials, CEQUA improved total corneal staining after just 14 days.16
Dr. White: Dr. Parekh, you raise an interesting point. How does the treatment of dry eye fit into your surgical considerations?
Dr. Parekh: In a recent study/survey of its members, the American Society of Cataract and Refractive Surgery (ASCRS) found that more than 90% of clinical study respondents felt that mild-to-moderate DED impacts the postoperative satisfaction of our patients after cataract and refractive surgery.18 So, it’s incredibly important to pause, to appropriately diagnose, and to treat these patients preoperatively. If they don’t have ocular surface issues, then I proceed to surgery. But if patients do have signs and symptoms of DED, and fluctuating vision is usually a sign of an ocular surface issue, then I rehabilitate the corneal surface and wait for them to get better. When I use a product like CEQUA, I may see the benefit within a couple of weeks.
Dr. McGee: As an optometrist, it’s so important to me to optimize a patient’s ocular surface before I send him or her to my ophthalmic partners for surgery. If I can improve total corneal staining and stabilize the tear film, then all the patient’s data are optimal before he or she enters the OR. Failure to treat the ocular surface before surgery means that that patient will need more extensive optometric care postoperatively, and it can limit a patient’s best visual outcome. Having data that show that I can improve a patient’s corneal surface in just 14 days, before he or she schedules the initial surgical consultation and undergoes preoperative measurements, is impressive.
Dr. Ayres: This is just the beginning of the dataset that has really changed our practice pattern for ocular surface optimization prior to any type of surgery, including cataract, cornea, refractive, and refractive cataract. What we’re looking for is speed of effect. We want the central cornea to look good, because that’s where keratometry data come from. What I like about the clinical trial data on CEQUA is that they included central corneal staining and total corneal staining—not conjunctival staining, and not just inferior corneal staining. Because of the corneal staining clinical trial data, I now reach for CEQUA for corneal optimization prior to surgery.
RELIEF OF SYMPTOMS
Dr. White: I’d like to talk a little more about symptom relief. Symptoms are often what motivate patients to seek help from an optometrist or ophthalmologist. Dr. Devries, what has been your experience, and what data does CEQUA have to support symptom relief?
Dr. Devries: Investigators in the clinical trials for CEQUA used the modified symptom assessment in dry eye (mSANDE) score, which is a visual analog scale on which patients score the severity of their symptoms between 0 and 100. On day 28, CEQUA patients’ SANDE score reporting showed a meaningful reduction from baseline in symptom severity within 1 month,12 and that is consistent with what I see in my clinic.
FORMULATION & IMPROVING SYMPTOMS
Dr. White: Let’s talk a little bit about improving DED patients’ visual acuity, because we’re in the vision game. Dr. McGee, tell us a little bit about the effects of CEQUA on patients’ vision.
Dr. McGee: As Dr. Ayres said, whether we’re doing a refraction for new spectacles, or fitting a contact lens patient, or evaluating someone for surgery, DED, or aesthetics, everybody is there to see better. These are unique data—statistically significant improvement in visual acuity.1,19 We don’t have this kind of data for any other dry eye prescription currently available.
In the clinical trial for Xiidra, investigators were looking at inferior corneal staining as one of the primary efficacy endpoints.20 In the CEQUA clinical trial, patients’ improvement in central corneal staining became statistically significant at 2 months (Figure 3). Better central corneal staining correlated to better visual acuity.17
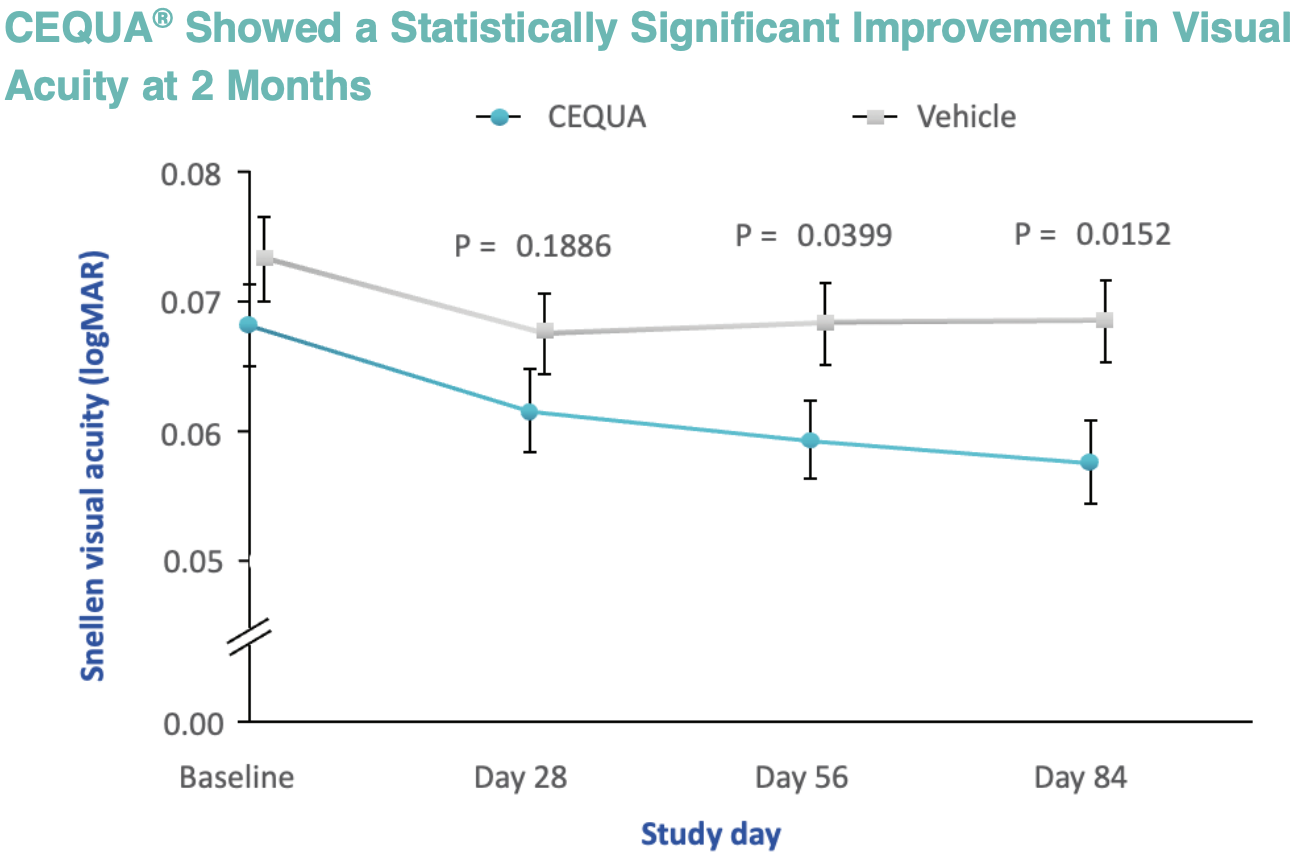
Figure 3. In a pooled analysis of phase 2b/3 and phase 3 clinical studies, CEQUA showed a statistically significant improvement in visual acuity at 2 months, which correlated with reduced central corneal staining as early as day 56.1,17,19 (Note: a lower Snellen logMAR value indicates better visual acuity.)
Dr. Ayres: CEQUA gives us a therapy that starts to act on the cornea within 2 weeks. It improves symptom scores within a month. It clears the central cornea, and that’s where our keratometry data come from. When it comes to surgical optimization, that central cornea is critical. We physicians want a tolerable medication that works in as little as 2 weeks, which is relatively quickly. Patients want better vision. CEQUA delivers on both.
Dr. White: Dr. Ayres, we’ve seen some impressive clinical data on CEQUA, but the issue is not impressive data, but rather patients who discontinue the medicines we prescribe in the real world. Do the clinical data on CEQUA alone provide a reason to think we’ll get any different result than what we’ve seen historically?
Dr. Ayres: Based on past experience, no! In the past, I’ve seen good data from clinical trials and have wondered what I could expect in the real world when I would prescribe patients a drug. Also, I have had the thought: what if I could actually see what my patients do when I give them a prescription and don’t see them back for many months or even a year later? Well, now I have an answer. Figure 4 shows results from an analysis of a national provider-based claims database, from which investigators evaluated the adherence rates of the three main ocular surface medications: CEQUA, Restasis, and Xiidra.1 Over the course of 1 year, CEQUA patients stayed on treatment longer than patients who received Xiidra or Restasis. I think these data influence me quite a bit when I’m thinking about what I will prescribe for my patients.
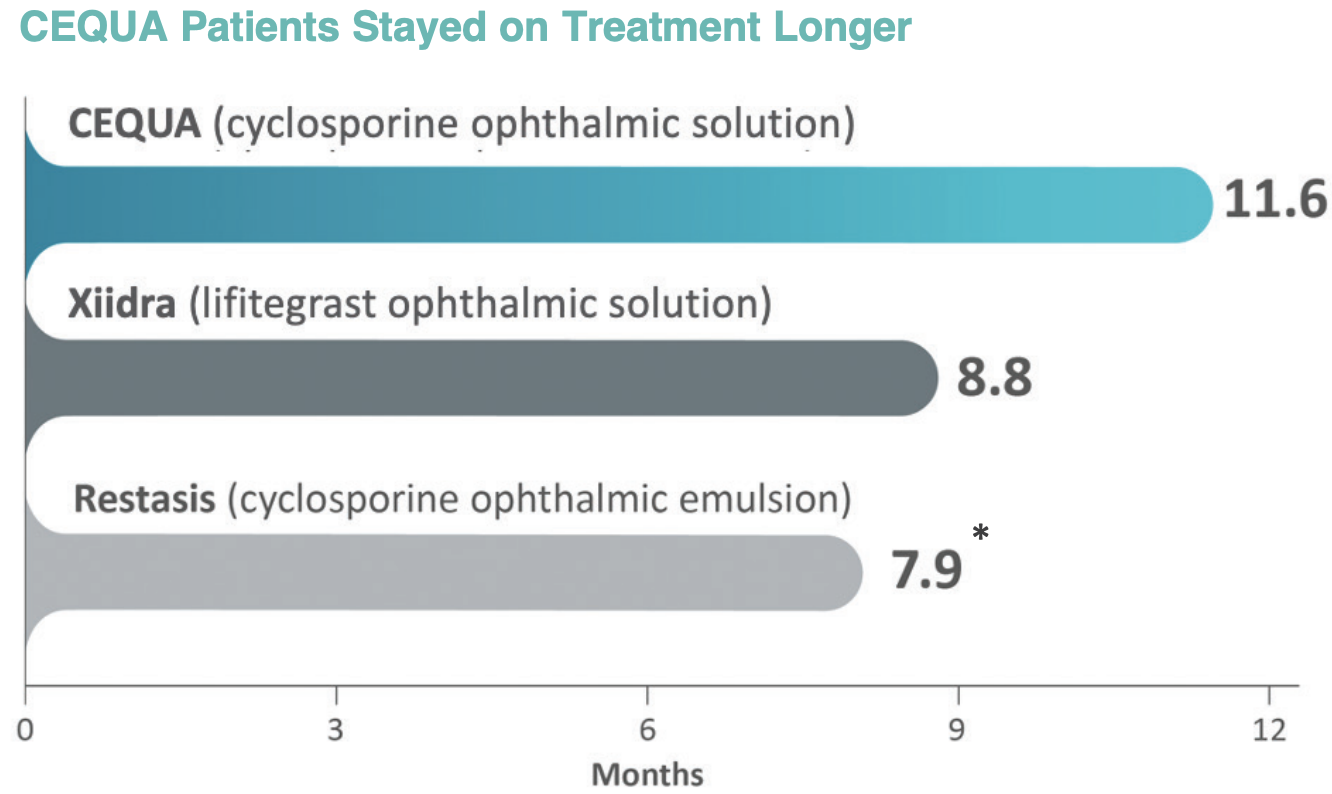
Figure 4. The median treatment duration for three prescription DED drops per the results of a real-world, retrospective, longitudinal cohort study of data from the Symphony Health Integrated Dataverse (IDV), a national provider-based claims database. It examined time to treatment discontinuation, probability of treatment discontinuation, and treatment persistence among patients with DED treated with CEQUA (n=1,846), Restasis (n=2,248), or Xiidra (n=3,008).1 After 360 days, more patients were still using CEQUA than Xiidra and Restasis. (*Statistically significant difference in favor of CEQUA.)
SUMMARY & CONCLUSIONS
Dr. White: Let’s each share one key thing that stands out about the data we’ve shared today, and how you feel that information may influence the way that you will treat DED patients with CEQUA.
Dr. Ayres: The data point that changed my practice pattern was the ability of CEQUA to improve central corneal staining in as little as 2 weeks. That finding makes me say, “This is what I want to use for my patients.”
Dr. McGee: My deciding factor was the data showing that CEQUA can improve visual acuity. I refract, I fit contact lenses, I treat patients with glaucoma, I treat dry eye. When I can enhance visual acuity by improving central corneal staining, that’s the big differentiator for me.
Dr. Devries: The feature that stands out to me is the total corneal clearing that leads to faster visual improvement in central visual acuity.
Dr. Parekh: We are all visual health professionals, and therefore our job is to protect, preserve, and enhance vision. The fact that an eye drop improves central corneal clearing within a couple of months, and that it begins working within a couple of weeks, is incredibly impressive and highly differentiated.
Dr. Johnston: For me, it’s the speed of onset with CEQUA, that total corneal clearing was seen at 2 weeks. That’s what I’m most impressed with in the clinical data we have seen.
Dr. White: The thing that’s most impressive to me—the key differentiator for CEQUA—is its method of delivery. The fact that the nanomicellar encapsulation is able to deliver the hydrophobic cyclosporine molecule into the tissues where it needs to work explains why it’s so tolerable, has so few side effects, and works after just 14 days. The penetration of CEQUA is up to three times greater than at least one other cyclosporine preparation in the ocular surface tissues. As Dr. Parekh said, cyclosporine is the most studied molecule in the anterior segment. How is CEQUA able to achieve the advantages of rapid onset and high tolerability? I think it’s that nanomicellar encapsulation, the delivery vehicle.
1. Karpecki P, Barghout V, Schenkel B, et al. A retrospective analysis of real-world treatment patterns in patients with dry eye disease receiving CEQUA, Restasis, or Xiidra. Poster presented at AMCP Nexus; October 11-14, 2022; National Harbor, MD.
2. Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438-510.
3. Stevenson W, Chauhan SK, Dana R. Dry eye disease: an immune-mediated ocular surface disorder. Arch Ophthalmol. 2012;130(1):90-100.
4. Stern ME, et al. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Cornea. 1998;17(6):584-589.
5. Dartt DA. Dysfunctional neural regulation of lacrimal gland secretion and its role in the pathogenesis of dry eye syndromes. Ocul Surf. 2004;2(2):76-91.
6. White DE, Zhao Y, Ogundele A, et al. Real-world treatment patterns of cyclosporine ophthalmic emulsion and lifitegrast ophthalmic solution among patients with dry eye. Clin Ophthalmol. 2019;22;13:2285-2292.
7. Mah F, Milner M, Yiu S, et al. PERSIST: Physician’s Evaluation of Restasis Satisfaction in Second Trial of topical cyclosporine ophthalmic emulsion 0.05% for dry eye: a retrospective review. Clin Ophthalmol. 2012;6:1971-1976.
8. US Patent 9,937,225 B2.
9. Cholkar K, Gilger BC, Mitra AK. Topical, aqueous, clear cyclosporine formulation design for anterior and posterior ocular delivery. Transl Vis Sci Technol. 2015;4(3):1-16.
10. Mandal A, Bisht R, Rupenthal ID, Mitra AK. Polymeric micelles for ocular drug delivery: From structural frameworks to recent preclinical studies. J Control Release. 2017;248:96-116.
11. Cholkar K, Patel A, Vadlapudi AD, Mitra AK. Novel nanomicellar formulation approaches for anterior and posterior segment ocular drug delivery. Recent Pat Nanomed. 2012;2(2):82-95.
12. Data on file. Cranbury, NJ: Sun Pharmaceutical Industries, Inc.
13. Weiss SL, William GK. Ocular distribution of cyclosporine following topical administration of OTX-101 in New Zealand white rabbits. J Ocul Pharmacol Ther. 2019; 35(7):395–402.
14. Tauber J, Schechter BA, Bacharach J, et al. A Phase II/III, randomized, double-masked, vehicle-controlled, dose-ranging study of the safety and efficacy of OTX-101 in the treatment of dry eye disease. Clin Ophthalmol. 2018;12:1921-1929.
15. CEQUA [package insert]. Cranbury, NJ: Sun Pharmaceutical Industries, Inc.; 2022.
16. Schechter BA, Urbieta M, Bacharach J, et al. Effect of OTX-101 in patients with dry eye disease at day 14 of treatment: ocular surface endpoint results from the phase 2b/3 clinical trial. Clin Ophthalmol. 2022:16:4145-4151.
17. Malhotra R, Devries DK, Luchs J, et al. Effect of OTX-101, a novel nanomicellar formulation of cyclosporine a, on corneal staining in patients with keratoconjunctivitis sicca: a pooled analysis of phase 2b/3 and phase 3 studies. Cornea. 2019;38:1259-1265.
18. Starr CE, Gupta PK, Farid M, et al. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. J Cataract Refract Surg. 2019;45(5):669-684.
19. Goldberg DF, Malhotra RP, Schechter BA, et al. A phase 3, randomized, double-masked study of otx-101 ophthalmic solution 0.09% in the treatment of dry eye disease. Ophthalmology. 2019;126(9):1230-1237.
20. Tauber J, Karpecki P, Latkany R, et al. Lifitegrast ophthalmic solution 5.0% versus placebo for treatment of dry eye disease: results of the randomized phase III opus-2 study. Ophthalmology. 2015;122(12):2423-2431.






INDICATIONS AND USAGE
CEQUA® (cyclosporine ophthalmic solution) 0.09% is a calcineurin inhibitor immunosuppressant indicated to increase tear production in patients with keratoconjunctivitis sicca (dry eye).
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Potential for Eye Injury and Contamination: To avoid the potential for eye injury and contamination, advise patients not to touch the vial tip to the eye or other surfaces.
Use with Contact Lenses: CEQUA should not be administered while wearing contact lenses. If contact lenses are worn, they should be removed prior to administration of the solution. Lenses may be reinserted 15 minutes following administration of CEQUA ophthalmic solution.
ADVERSE REACTIONS
The most common adverse reactions reported in greater than 5% of patients were pain on instillation of drops (22%) and conjunctival hyperemia (6%). Other adverse reactions reported in 1% to 5% of patients were blepharitis, eye irritation, headache, and urinary tract infection.
Please see Full Prescribing Information.
CEQUA and NCELL are registered trademarks of Sun Pharmaceutical Industries Limited. All other trademarks are the property of their respective owners. PM-US-CQA-1449 01/2024
Important Safety Information
INDICATIONS AND USAGE
CEQUA® (cyclosporine ophthalmic solution) 0.09% is a calcineurin inhibitor immunosuppressant indicated to increase tear production in patients with keratoconjunctivitis sicca (dry eye).
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Potential for Eye Injury and Contamination: To avoid the potential for eye injury and contamination, advise patients not to touch the vial tip to the eye or other surfaces.
Use with Contact Lenses: CEQUA should not be administered while wearing contact lenses. If contact lenses are worn, they should be removed prior to administration of the solution. Lenses may be reinserted 15 minutes following administration of CEQUA ophthalmic solution.
ADVERSE REACTIONS
The most common adverse reactions reported in greater than 5% of patients were pain on instillation of drops (22%) and conjunctival hyperemia (6%). Other adverse reactions reported in 1% to 5% of patients were blepharitis, eye irritation, headache, and urinary tract infection.
Please see the Full Prescribing Information.


