
Capsulotomy is a foundational step in cataract surgery. Achieving an efficient, reproducible, effective, and inexpensive capsulotomy may prove challenging for some surgeons. Although femtosecond laser–assisted cataract surgery (FLACS) may be appealing to patients and imply a degree of automation, only 8% of patients actually undergo the procedure.1 Surgeons have reported a lack of FLACS-specific outcomes data and decreased surgical efficiency as barriers to implementation of this technology.1 Some surgeons may prefer to perform manual capsulorhexis, also called continuous curvilinear capsulorhexis (CCC), due to the efficiency and reduced expense of the procedure. However, associations with anterior capsule radial tears,2 rhexis breach,2 dysphotopsia,3 and compromised retinal images3 make CCC, while perhaps less disruptive than FLACS, less reliable as a reproducible method of capsulorhexis creation.
Surgeons seeking the efficiency and price point of CCC and the engineering elegance and reproducibility of FLACS may consider turning to the use of precision pulse capsulotomy (PPC) with Zepto (Centricity Vision). The recently upgraded Zepto improves on the precision and mechanics of the previous generation while still allowing surgeons to take the same approach to efficient, effective capsulotomy creation.
A QUICK SUMMARY OF ZEPTO’S USE
Zepto is inserted into an incision 2.2 mm or greater, after which the device’s pushrod is retracted to allow the re-formation of Zepto’s circular suction cup and nitinol ring. The suction cup fully applanates onto the anterior capsule. Once positioned, 12 micropulses of energy are applied in 4 milliseconds and a 5.2-mm median diameter capsulotomy is formed. During the energy release, BSS is trapped between the nitinol ring and the anterior chamber, undergoing a phase change to a gaseous state (high-pressure steam), thereby creating a capsulotomy. Suction is reversed and OVD is pushed back into the suction cup with a small amount of BSS, floating the Zepto tip off the capsule. From there, the device is withdrawn and cataract surgery proceeds per the surgeon’s typical protocols.
WHAT’S NEW WITH THE NEXT GENERATION OF ZEPTO?
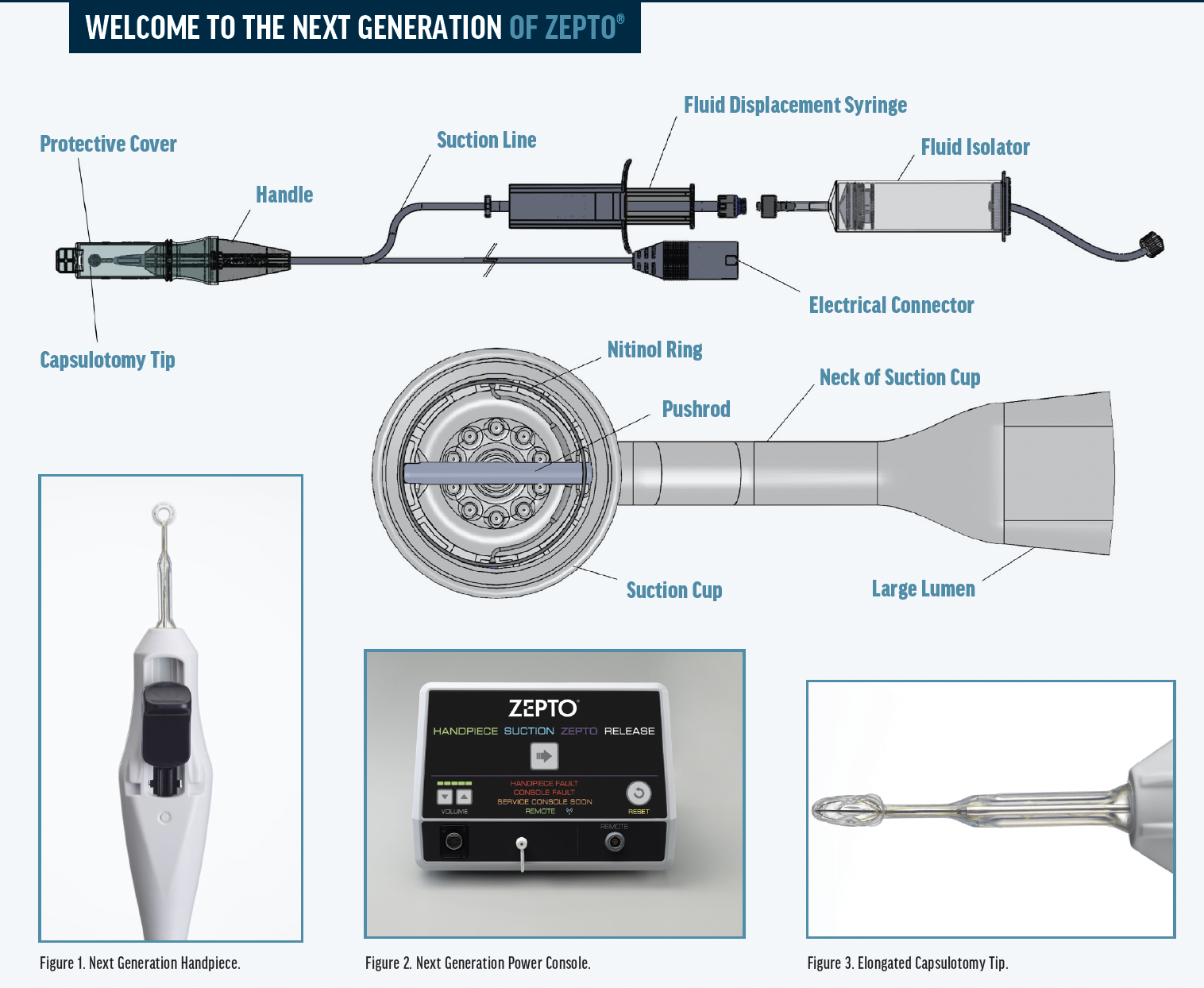
Centricity Vision’s commitment to incorporating surgeon feedback means that Zepto is constantly improving. The most recent advances of the Next Generation Zepto Cataract System make the device more precise and efficient through improvements in multiple device components. (For a graphic depiction of these innovations, see the illustration on page 2 and Figures 1-3).
Handpiece Design
Several enhancements lead to major improvements to the handpiece design in the Next Generation Zepto. The smoother, more ergonomic finger slide allows a comfortable grip. Improved designs of items such as the release dispenser (which now permits more consistent suction) and the addition of a luer-activated one-way valve (thus removing a step from the procedure itself) resulted in improved efficiency and a shorter learning curve.
Nitinol Ring
With the Next Generation nitinol ring design, the 12 micropulses of energy released by the nitinol ring are applied more consistently, thereby creating a uniformly strong and symmetrical 360° capsulotomy, eliminating the concerns associated with previous models.
Suction Cup
Creating and maintaining suction prior to applying energy is one of the most important steps to a successful Zepto capsulotomy. By adding five flow holes to the baffle of the suction cup, the Next Generation Zepto device improves the flow dynamics of various OVDs to the sub-incisional region and reduces roughness of the capsulotomy edge. The result is a strong and uniform 360° capsulotomy.
Power Console
Underlying all of the improvements to the Next Generation Zepto Cataract System is the improved power console. The new power console employs a single button to advance from suction to energy initiation and offers voice-guided prompts. The console’s ability to run a self-test allows the unit to adjust its output voltage to deliver consistent energy regardless of resistance.
THE CASE FOR ZEPTO
Our subjective experience, while useful to share with fellow surgeons, may be an insufficient foundation for adopting Zepto into clinical practice. However, there is robust peer-reviewed literature that outlines the benefits of PPC compared with CCC.
Gundersen et al performed a retrospective chart review of 243 eyes undergoing cataract surgery or refractive lens exchange with either PPC or CCC used during capsulorhexis creation.4 They found that the group undergoing PPC had significantly more patients with minimal residual refractive cylinder (≤ 0.50 D) compared to those who had received CCC (89% vs 79%, P = .03). Although the rate of capsulotomy-related complications was not statistically significant among the two groups, the complication rate was 4.1% among those who had received PPC compared with 6.6% among those who had undergone CCC.
BOOTS ON THE GROUND
Want to hear from high-volume Zepto (Centricity Vision) users about how this technology has positively affected their patient outcomes and OR workflow? Check in here with three Zepto experts.

Mark C. Vital, MD
Houston Eye Associates
Houston
“Zepto consistently delivers fast, reliable, round, durable, and central capsulotomies that outperform manual and femtosecond laser–assisted capsulotomies in both routine
and complex cases. Zepto is portable, simple, and a fraction of the cost of femtosecond platforms. Great for patients, great for surgeons, and an easy decision.”

Philip C. Roholt, MD
Roholt Vision Institute
North Canton, Ohio
“I’ve used Zepto since FDA 510(K) clearance in 2017. I find that patient fixation is excellent for capsulotomy centration, a feature not available with any other device, including femtosecond lasers. Zepto is easy to use under various conditions, including in patients with shallow chambers and in scenarios with poor capsular visibility due to cortical or dense cataract. Variations in globe or conjunctival anatomy do not limit the use of Zepto. It is my instrument of choice for white cataracts, as it helps avoid creation of the Argentinian flag sign.”

Becky J. Fredrickson, MD, PhD
Houston Eye Associates
Houston
“Zepto is an excellent tool for creating precise, round capsulotomies. It is straightforward to use with a minimal learning curve. Its portability allows for easy transport between operating rooms, thereby aiding efficiency.”
It should be noted that PPC is appropriate for more than just routine cases. Ifantides et al, in their review of 337 cataract surgery videos of routine and challenging cases that used PPC, reported that “PPC was useful in cases with multiple comorbidities that challenge capsulotomy performance,” including traumatic cataracts with compromised anterior and posterior capsules, intumescent cataracts in patients with constricted pupils, and in cases of penetrating keratoplasty using open-sky extracapsular cataract extraction.5 Of the cases using PPC that Ifantides et al reviewed, 99.4% resulted in free-floating capsulotomy with a mean capsulotomy diameter of 5.0 mm. They also reported excellent circularity of the capsulotomy, observing a mean ovality rate of only 3.0% and 360° capsular overlap in 98% of cases using PPC.
Still, PPC remains an effective tool for routine cataract surgery, and contributes to increased surgical efficiency. Thompson described a streamlined method of IOL centration on a patient’s visual axis that included the use of PPC.6 In his case series report, Thompson described that 86 patients undergoing routine cataract surgery with placement of a monofocal or multifocal IOL had the PPC device centered on the first Purkinje image as it became aligned with the fourth Purkinje image. It was reported that all patients fixated as instructed and all patients received an individualized PPC capsulotomy anchored on their specific visual axis. Thompson concluded that use of individualized PPC as a reference marker for IOL implantation on the visual axis may provide benefit to cases involving toric, multifocal and other IOLs.
In 2021, Thompson et al expanded on the particulars of PPC and emphasized that IOL positioning and stability is foundational to long-term satisfaction among cataract surgery patients.7 Zepto can be key to proper IOL placement (and therefore long-term patient satisfaction), with the authors noting that “with methods of automated capsulotomy and intraoperative capsulotomy centration, one can control the IOL position in the bag by an optimally located capsulotomy.”7
TRANSITIONING TO PPC FOR CAPSULOTOMY CREATION
Cataract surgeons who have yet to adopt Zepto’s PPC may find the device to be one of the most versatile technologies in their surgical armamentarium. Peer-reviewed literature has supported adoption of this new-era technology in routine and premium cataract surgery, as well as complex cases. Those who wish to rely on the latest surgical innovations while preserving efficacy, maintaining efficiency, and keeping costs under control may find that Zepto meets their demands for modern cataract surgery.
To learn more about how Zepto works, visit ZeptoZone.com.
1. Global Trends in Ophthalmology and the American Society of Cataract and Refractive Surgery. ASCRS Clinical Survey 2016.
2. Olali CA, Ahmed S, Gupta M. Surgical outcome following breach rhexis. Eur J Ophthalmol. 2007;17:565-570.
3. Wirtitsch MG, Findl O, Menapace R, et al. Effect of haptic design on change in axial lens position after cataract surgery. J Cataract Refract Surg. 2004;30:45-51.
4. Gundersen KG, Potvin R. Clinical results after precision pulse capsulotomy. Clin Ophthalmol. 2020;14:4533-4540.
5. Ifantides C, Lee J, Rouweyha R, Vital M, Sretavan D. Precision pulse capsulotomy: performance metrics and utility in routine and complex cases. J Cataract Refract Surg. 2020;46(11):1522-1529.
6. Thompson V. Streamlined method for anchoring cataract surgery and intraocular lens centration on the patient’s visual axis. J Cataract Refract Surg. 2018;44(5):528-533.
7. Thompson V, Holladay J, Sretavan D. Use of P1-P4 Purkinje reflections as a surrogate sign for intraoperative patient fixation. J Cataract Refract Surg. 2021;47(12):e60-e65.

