


Blepharitis—a common ocular condition characterized by inflammation of the eyelids—can have various etiologies (see 10 Causes of Blepharitis). Demodex infestation is a significant contributor to blepharitis and affects approximately 25 million individuals in the United States.1 Demodex blepharitis (DB) presents unique challenges for diagnosis and management.1 This article explores DB’s etiology and clinical presentation, diagnostic methods, treatment options, and preventive measures.
10 CAUSES OF BLEPHARITIS
Understanding the different causes of blepharitis1 is crucial for accurate diagnosis and effective management.
No. 1: Staphylococcal blepharitis
This condition is usually associated with anterior blepharitis due to staphylococcal bacteria, particularly Staphylococcus aureus. Patients with staphylococcal blepharitis frequently present with symptoms such as crusty, red eyelids and irritation along the eyelid margins.
No. 2: Seborrheic blepharitis
This form of blepharitis is associated with seborrheic dermatitis, a chronic inflammatory skin condition that can affect the eyelids. Patients with seborrheic blepharitis may exhibit greasy, flaky scales on the eyelid skin as well as redness and itching.2
No. 3: Meibomian gland dysfunction
Dysfunction of the meibomian glands contributes to posterior blepharitis. Exam findings include meibomian gland obstruction, altered lipid composition of the tear film, and symptoms of evaporative dry eye disease.
No. 4: Demodex infestation
Demodex mites, specifically Demodex folliculorum and Demodex brevis, can proliferate within the eyelash follicles and sebaceous glands, leading to Demodex blepharitis. Patients may experience itching, burning, redness, and cylindrical dandruff (collarettes) along the base of the eyelashes.3
No. 5: Allergic blepharitis
Reactions to environmental allergens such as pollen, pet dander, and cosmetic products (including fake eyelashes) can cause allergic blepharitis. Patients with this condition usually present with itching, tearing, eyelid swelling, and conjunctival injection.
No. 6: Rosacea-associated blepharitis
Patients with rosacea, a chronic inflammatory skin condition, may develop blepharitis as a component of ocular rosacea. These individuals often exhibit ocular irritation, redness, and eyelid telangiectasia.3
No. 7: Contact lens–related blepharitis
Prolonged contact lens wear, improper lens hygiene, and allergic reactions to lens materials can all trigger blepharitis. These patients generally present with lens discomfort, red eyes, and papillary conjunctivitis.
No. 8: Malassezia infection
This genus of yeast-like fungi can contribute to blepharitis, particularly in patients with seborrheic dermatitis. Individuals with Malassezia blepharitis may present with greasy scales, erythema, and pruritus along the eyelid margins.
No. 9: Viral blepharitis
Viral infections, such as herpes simplex virus and varicella zoster virus, can cause viral blepharitis. The presentation of vesicular lesions, pain, and erythema along the eyelid margins, often in a dermatomal distribution, signal a viral etiology.
No. 10: Bacterial infection
In addition to staphylococcal blepharitis, other bacterial infections, such as those caused by Streptococcus or Moraxella, can cause blepharitis. Patients with bacterial blepharitis may present with an acute onset of symptoms, including eyelid erythema, swelling, and purulent discharge. Sometimes, the condition is also associated with preseptal cellulitis.4
1. Eberhardt M, Rammohan G. Blepharitis. In: StatPearls [Internet]. January 23, 2023.
2. Cheng AM, Hwang J, Dermer H, Galor A. Prevalence of ocular demodicosis in an older population and its association with symptoms and signs of dry eye. Cornea. 2021;40(8):995-1001.
3. Fromstein SR, Harthan JS, Patel J, Opitz DL. Demodex blepharitis: clinical perspectives. Clin Optom (Auckl). 2018;10:57-63.
4. Zhang AC, Muntz A, Wang MTM, Craig JP, Downie LE. Ocular Demodex: a systematic review of the clinical literature. Ophthalmic Physiol Opt. 2020;40(4):389-432.
RESEARCH ON DB
Limited epidemiologic and demographic data on DB are available, owing in part to diagnostic challenges and a range of reported prevalence rates. Thankfully, a recent emphasis on DB is generating more information.
Demodex mites are ubiquitous and commonly found in the general population. Research using a variety of diagnostic methods has reported prevalence rates ranging from approximately 23% to 100% in adults.2 One study found that the prevalence of Demodex increased with age; more than 80% of patients older than 60 years of age and 100% of those older than 70 years of age were affected.3 The statistics are astonishing but reflect my own anecdotal observations in clinical practice.
The incidence of Demodex infestation is equal in men and women.4 Hormonal factors and differences in facial sebum production between the sexes may contribute to variations in Demodex prevalence. Risk factors associated with DB include advanced age, diabetes, poor eyelid hygiene, a compromised immune system, certain systemic conditions (eg, rosacea) and medications (eg, immunosuppressive therapy), and ocular surface disease. Individuals with a history of chronic blepharitis, meibomian gland dysfunction (MGD), or ocular inflammation may be at increased risk of Demodex infestation.1
DB is caused by microscopic parasites, Demodex folliculorum and Demodex brevis, that infest the eyelids. The parasites preferentially inhabit the hair follicles and sebaceous glands of the eyelids, causing a variety of ocular symptoms and inflammation. Patients who have DB typically present with symptoms such as itching, burning, foreign body sensation, and redness and crusting of the eyelids. Most cases of DB are mild and self-limiting. Moderate to severe disease can lead to complications such as MGD, punctate epithelial erosions, keratitis, and secondary infection.
DIAGNOSIS
Clinical examination. Although obtaining a thorough patient history is important, a lack of ocular symptoms does not mean that no infestation is present. A comprehensive clinical examination of the eyelids and ocular surface is the first step toward diagnosing DB. Look for eyelid margin abnormalities such as cylindrical dandruff (collarettes), telangiectasia, and thickening. The Titan study, a multicenter retrospective chart review, found that 58% of 1,032 consecutive patients (and 69% of those with a blepharitis diagnosis) presented with collarettes (Figure 1).5-7 It can be helpful to ask patients to look downward during the slit-lamp examination. This exposes the anterior surface of the eyelids, the eyelid margin, and the base of the eyelash hair follicle.
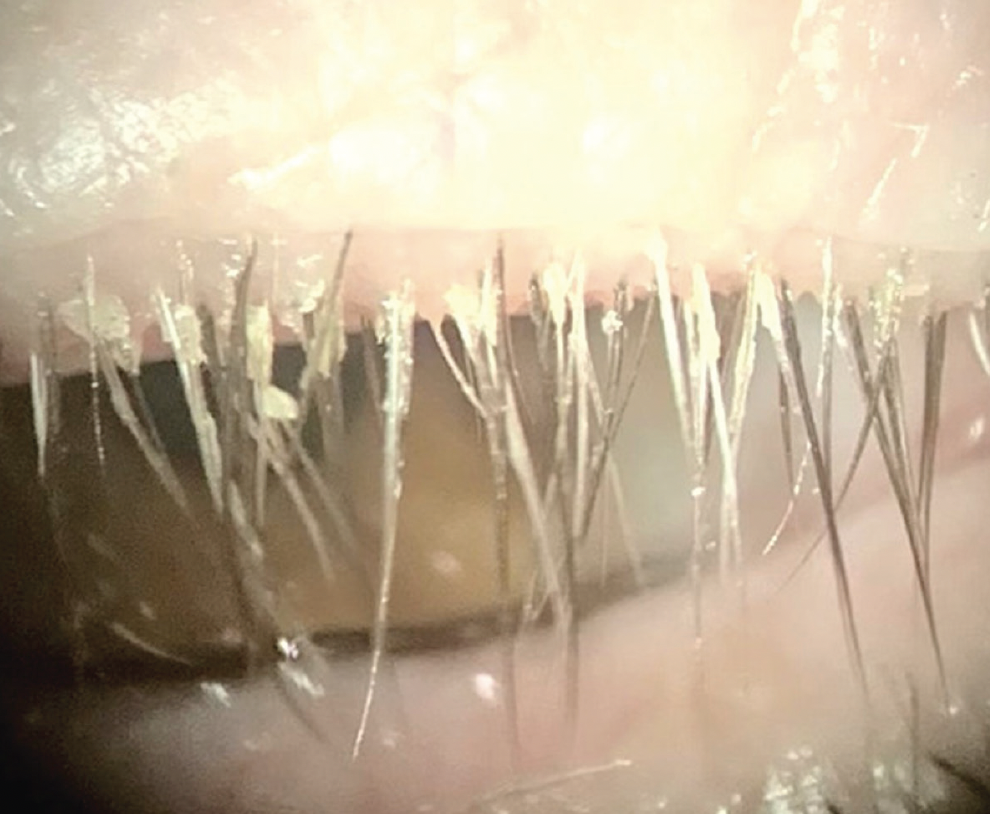
Figure 1. Collarettes, the pathognomonic sign of DB, are readily visible at the base of the upper lash margin on downward gaze at the slit lamp.1
Symptoms. The most common—and most bothersome—symptom associated with DB is ocular itching.8,9 Demodex-related itching most often occurs at night and early in the morning after periods of mite activity.8 The timing helps to distinguish DB from ocular allergy, for which itching is usually worst during the day. Dry eye and blepharitis patients who have Demodex are significantly more likely to report itching than those who do not have the mites, and the frequency of itching complaints increases with higher Demodex density.1,10 Individuals with dry eye or blepharitis who report itching are 2.6 times more likely to have Demodex.11
Visualization. In vivo confocal microscopy allows direct visualization of Demodex mites and their movement within the eyelid structures (Figure 2). This noninvasive imaging technique can provide valuable insight into the extent of infestation and help guide diagnosis and treatment decisions.

Figure 2. D folliculorum is found on human skin, especially the cheeks, nose, and eyelids.1
(Both images courtesy of Patrick Vollmer, OD)
Epilation of the eyelashes followed by a microscopic examination of collected samples can confirm the presence of the mites. This method also allows direct visualization and provides quantitative information about Demodex density. Ideally, the epilation of multiple eyelashes from different regions of the eyelid is performed.12 Unfortunately, this technique is impractical outside of clinical trials.
In my experience, determining the presence or absence of collarettes at the slit lamp often suffices for the diagnosis of DB in clinical practice.
MANAGEMENT
Treatment options. The treatment of DB requires a multifaceted approach. Meticulous lid hygiene is the cornerstone of management. Advise patients to clean their eyelids regularly with warm compresses and gentle eyelid scrubs to remove excess debris, crust, and Demodex mites. Several oral, topical, and device-based hygiene options have been evaluated in studies and are in use clinically, but none has been approved by the FDA for the treatment of DB.1
Historically, various topical agents, such as tea tree oil (TTO) and azithromycin, have been used to treat Demodex mites and temporarily alleviate patients’ symptoms. Gels, shampoos, ointments, and lid wipes containing various concentrations (3%–100%) of TTO have been shown to be effective at improving the signs and symptoms of blepharitis.13 The products’ efficacy for mite eradication, however, remains uncertain.14 Products with high concentrations (> 50%) of TTO have greater effectiveness, but they are not considered safe for home use and must be applied in the clinic.15 Highly concentrated TTO is toxic to the meibomian glands and ocular surface, and it does not completely eradicate Demodex.
Refractory or severe DB has traditionally been treated with oral medications such as ivermectin and azithromycin. The medications target the mites systemically to improve control of the infestation, but relief is often temporary. Meibomian gland expression, thermal pulsation therapy, and intense pulsed light therapy have also been employed to complement conventional, conservative treatment by addressing underlying MGD and inflammation.
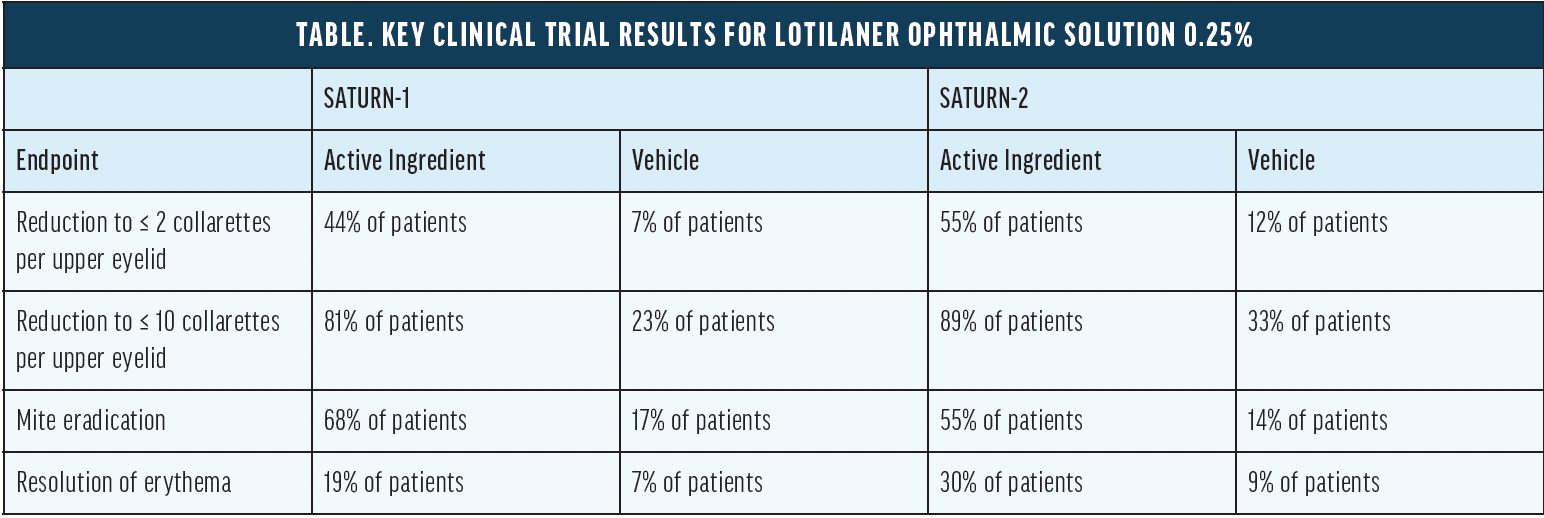
The recent FDA approval of lotilaner ophthalmic solution 0.25% (Xdemvy, Tarsus Pharmaceuticals) could revolutionize DB management. Most of the other forms of treatment discussed in this article are targeted toward controlling the symptoms caused by mite infestation. In contrast, lotilaner ophthalmic solution acts specifically via mite GABA-gated chloride channels to launch a targeted attack that eventually kills the parasites. The Table shows several key results from the SATURN-1 and SATURN-2 clinical trials.16 In the trials, the most common adverse reaction was stinging and burning at the instillation site (10% of patients). Of note, no contraindications to treatment with lotilaner ophthalmic solution have been reported.
Prevention. Patient education and compliance play a crucial role in preventing DB recurrence. When counseling patients, emphasize the importance of consistent lid hygiene practices and adherence to prescribed treatment regimens. Explain that, even after eradication of the mites, reinfestation may occur, requiring treatment. To help prevent DB recurrence, advise patients to avoid the prolonged use of makeup, eyelash extensions, and contaminated cosmetics.
Periodic follow-up visits are essential for monitoring patients’ response to treatment, assessing the efficacy of interventions, and identifying signs of disease recurrence and complications.
1. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49(8):311-318.
2. Zhang AC, Muntz A, Wang MTM, Craig JP, Downie LE. Ocular Demodex: a systematic review of the clinical literature. Ophthalmic Physiol Opt. 2020;40(4):389-432.
3. Cheng AM, Sheha H, Tseng SC. Recent advances on ocular Demodex infestation. Curr Opin Ophthalmol. 2015;26(4):295-300.
4. Biernat MM, Rusiecka-Ziółkowska J, Piątkowska E, Helemejko I, Biernat P, Gościniak G. Occurrence of Demodex species in patients with blepharitis and in healthy individuals: a 10-year observational study. Jpn J Ophthalmol. 2018;62(6):628-633.
5. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153-1164.
6. Luo X, Li J, Chen C, Tseng S, Liang L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;36(suppl 1):S9-S14.
7. Rabensteiner DF, Aminfar H, Boldin I, et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am J Ophthalmol. 2019;204:7-12.
8. Ayres BD, Donnenfeld E, Farid M, et al. Clinical diagnosis and management of Demodex blepharitis: the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). Eye (Lond). 2023;37(15):3249-3255.
9. O’Dell L, Dierker DS, Devries DK, et al. Psychosocial impact of Demodex blepharitis. Clin Ophthalmol. 2022;16:2979-2987.
10. Cheng AM, Hwang J, Dermer H, Galor A. Prevalence of ocular demodicosis in an older population and its association with symptoms and signs of dry eye. Cornea. 2021;40(8):995-1001.
11. Sędzikowska A, Osęka M, Grytner-Zięcina B. Ocular symptoms reported by patients infested with Demodex mites. Acta Parasitol. 2016;61(4):808-814.
12. Luo KS, Xie A, Yang JJ, Shen EP. Critical value of Demodex count per lash for symptomatic and clinical improvement of Demodex blepharitis. Eye (Lond). 2022;36(3):663-665.
13. Karakurt Y, Zeytun E. Evaluation of the efficacy of tea tree oil on the density of Demodex mites (Acari: Demodicidae) and ocular symptoms in patients with demodectic blepharitis. J Parasitol. 2018;104(5):473-478.
14. Savla K, Le JT, Pucker AD. Tea tree oil for Demodex blepharitis. Cochrane Database Syst Rev. 2020;6(6):CD013333.
15. Cheung IMY, Xue AL, Kim A, Ammundsen K, Wang MTM, Craig JP. In vitro anti-demodectic effects and terpinen-4-ol content of commercial eyelid cleansers. Cont Lens Anterior Eye. 2018;41(6):513-517.
16. Saturn-2 Study Group; Gaddie IB, Donnenfeld ED, Karpecki P, et al. Lotilaner ophthalmic solution 0.25% for Demodex blepharitis: randomized, vehicle-controlled, multicenter, phase 3 trial (Saturn-2). Ophthalmology. 2023;130(10):1015-1023.

