
Many cataract and refractive surgeons are supremely confident in their ability to execute precise, elegant manual surgery. Still, as we strive to advance >procedures> and improve outcomes, many of us have embraced femtosecond laser–assisted cataract >surgery> (FLACS) to improve our precision, efficiency, and visual results while maintaining excellent safety standards.
In my practice, I placed the LenSx® Laser (Alcon) at the center of my FLACS procedures for several reasons. LenSx is the only platform to be trusted for use in over 3 million procedures and counting;1,2 this volume speaks to the platform’s ease of use and my colleagues’ confidence in the technology. The ability to create capsulotomies with LenSx, in my experience, is superior to that of manual surgery and has improved my surgical precision.3-5 Having the opportunity to titrate settings to various lens densities during fragmentation6 has made my surgery more predictable and efficient, and my OR schedule has been optimized so I can add more cases to my OR day. Visualizing the patient via the Verion® Image Guided System (Alcon) allows digital overlay of a surgeon’s operative plans, as well as guiding placements of incisions and arcuates and reduces the risk of transcription error. All of this empowers me to customize treatments to each specific patient and maximize outcomes for both the patient and myself as the surgeon.
A Deeper Dive Into FLACS With LenSx
Management of presbyopia and complex cases has become easier thanks to innovations in the IOL space, and many of our cataract patients now expect that we can surgically address low levels of astigmatism. The resulting increase in cataract patients’ visual and refractive demands requires surgeons to have more predictable outcomes, which can be achieved with more precise surgery. Surgeons seeking higher degrees of precision and predictability often turn to FLACS.
Good outcomes require precise capsulotomies and consistent postoperative anatomic outcomes. Compared with manual surgery, using LenSx can result in more precise, reliable, and reproducible capsulotomies.3-5 Use of LenSx has allowed 98.6% of capsulotomies to be achieved without manual separation of residual tags, 97.6% of corneal incision to be opened by a blunt spatula, and 99.5% of fragmentation to require no additional segmentation after the laser procedure.7
With LenSx, the outcomes speak for themselves. Compared with patients who have undergone manual surgery, patients whose procedures include LenSx are more likely to fall within 0.50 D of their target refraction (83.1% vs. 94.2%, respectively)8 and will experience 50.7% less mean postoperative astigmatism (0.65 D vs 0.32 D, respectively).8
Surgeons always keep an eye on safety, and the data support that using LenSx supports a safe surgery. The average time under suction for a routine, uncomplicated cataract case is less than 2 minutes when using LenSx.9 Patients experience 51% less phaco time10 and 43% less phaco energy10 compared with manual procedures when undergoing surgery with LenSx.
We cataract surgeons also value efficiency, and complicated cases that require a more careful approach can become inefficient if performed manually. In my subjective experience, the predictability of how the LenSx Laser will break up a cataract creates efficient surgeries compared with manual approaches in cases where uncommon conditions such as small pupil (Video 1) or a white swollen lens (Video 2) are present.
Watch it Now
Leveraging Laser Cataract Surgery in Eyes With Small Pupils
Dr. LaBorwit demonstrates the advantages of laser cataract surgery when managing cases of patients with small pupils.
Advantage of Femtosecond Laser Capsulotomy in White Swollen Lens
Swollen white cataracts are a significant challenge to any surgeon. In this video, Dr. LaBorwit explains the advantages of using the femtosecond laser during treatment.
LenSx is Always Improving
I was an early adopter of LenSx, deciding that it was a fit for my clinic within a year of it debuting in the US market. The platform has undergone a series of upgrades since arriving at my clinic, underscoring Alcon’s commitment to improvement and innovation of FLACS in general and LenSx in particular.
One of the most important upgrades was the addition of the SoftFit® Patient Interface (Alcon). SoftFit streamlines docking by obviating the use of liquids and the need to drain fluid between surgical steps. With SoftFit, docking requires only a single, hands-free step, empowering surgeons to better focus on patients. In my experience, surgical efficiency was noticeably improved after introduction of SoftFit. The updated configuration to the surgeon interface has made the user experience more intuitive, and improvements to intraoperative OCT imaging allow me to capture the anatomy of the entire anterior segment on a single scan without the hiccups of lag time associated with computer processing and imaging stitching. Advanced imaging also allows me to visualize lens density, arming me with reliable data for fragmentation.
Tips for LenSx Veterans
Surgeons whose experience with LenSx has left them comfortable with the technology are eligible to leverage the platform’s potential to make their clinic more efficient. I opt to let the LenSx Laser cut my patient’s nuclei into 20 pieces with a deep chop pattern (Figure 1), and I then bowl out the lens into 4 equal quadrants (Figure 2); other surgeons are free to take their own approaches when it comes to using LenSx to maximize their surgical prowess. Without the assistance of femtosecond laser, my lens removal approach would be untenable. I also rely on the technology to create a centered capsulotomy (which then aids in IOL centration and positively affects effective lens positioning) and guide arcuate placement, both of which are foundational to a desirable surgical outcome.
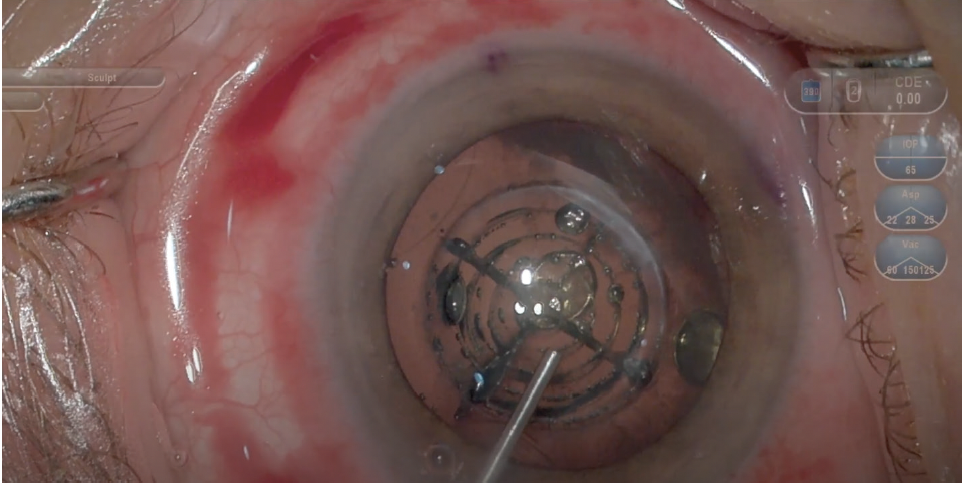
Figure 1. Use of the LenSx Laser allows me to cut the central 4.8 mm of the lens into 20 pieces. Here, a 5.0-mm capsulotomy and chop pattern at 5.3 mm are also depicted.
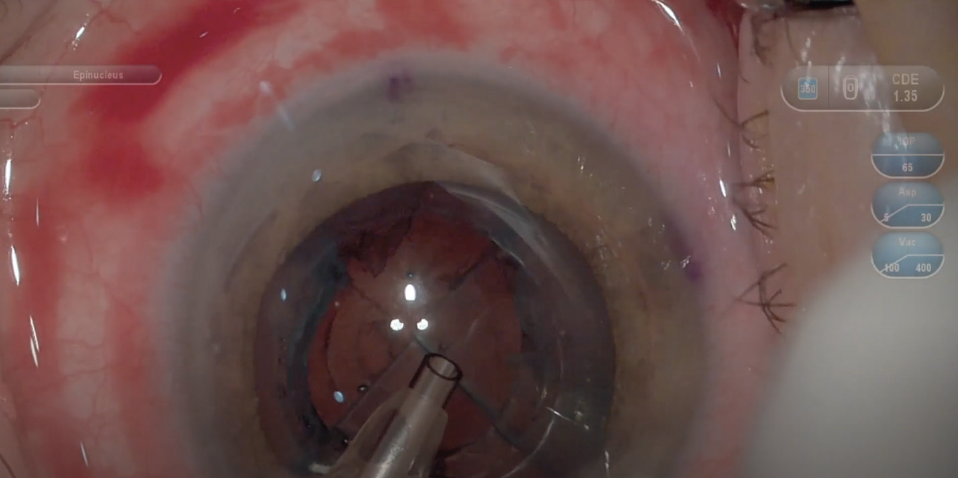
Figure 2. A 4-quadrant pattern is used to cut the cataract.

Increased efficiency can be applied to the overall OR, not just individual cases. Surgeons who are comfortable with LenSx might consider a hub-and-spoke surgical model, which has been shown to be more efficient than conventional surgical strategies.11 Switching to a hub-and-spoke paradigm may increase the number of cases allowed within a particular timeframe.
In my practice, I conduct roughly 30 cataract surgeries per day, approximately 20 of which use LenSx Laser technology. My team has created workflows that minimize downtime (eg, ensuring that turnover of one room occurs as I perform surgical steps in the other room) and maximize efficiency. When reconsidering how you might reorganize your OR scheduling, remember that LenSx is a tool that may help you unlock more efficiency.
What New Adopters Should Know
Surgeons who are adding LenSx to their surgical suite for the first time can rest well knowing that they are never locked into FLACS for every step—that is, if a surgeon determines that they want to forgo use of the laser in a specific step, they can always revert to manual surgery. For example, if an incision needs to be widened to accommodate a larger IOL, then a keratome could be used. Femtosecond laser can only add value to an OR and does not require that a new surgeon swap femtosecond technology for something with which they’re already familiar.
My first several cases with LenSx were straightforward, as the technology is intuitive, the docking is easy, and LenSx created free-floating capsulotomies with pristine edges.12 In my earliest days as a LenSx user, my first challenges occurred when I began to tinker with power and treatment patterns to optimize nuclear cuts and leverage the laser’s use in the OR during lens removal. Remember that resources such as Alcon’s clinical application support team can be tapped in these situations (and others) to offer guidance.
Over time, LenSx became a very powerful adjunct for my cataract surgical procedures. It was almost like I now had a “cheat code” for each FLACS case. I knew that LenSx would be an indispensable tool in my OR. Now that I am comfortable with this technology, I have significantly reduced the volume of CDE used in my procedures. Over the past 10 years, approximately 70% of my patients have choosen LenSx for their cataract surgery. This has allowed me to perform over 12,000 laser cataract cases with LenSx.
Surgeons who are new to FLACS platforms should spend time considering tactics for discussing this technology with patients. I feel obligated (as many of my peers do) to use laser technology when placing a premium IOL, and my conversations with premium IOL patients generally focus on how LenSx may allow for greater surgical precision, a reduction in energy used during surgery, and more predictable outcomes due to effective lens positioning and astigmatic keratotomies—all of which will maximize the potential of their chosen advanced-technology lens.
Use of laser in cataract surgery is typically a noncovered service for insurance policies, and patients set to receive a monofocal lens may wish to undergo surgery with LenSx to address corneal astigmatism. Many of these patients will consider including FLACS using a cost-benefit framework, and crafting useful responses to frequently asked questions will allow those conversations to flow smoothly. All of this is in service of educating patients about FLACS so they can make an informed decision—after all, they will only get to make this decision once. There is one important detail worth noting: you may be surprised how quickly patients grasp the concepts of FLACS. I educate patients about the benefits of FLACS so they are able to choose how I perform their surgical procedure. They’re paying attention, so make sure your explanations are clear, concise, and accurate.
Don’t underestimate how FLACS will build your practice’s reputation. I have received a significant number of referrals to my clinic from previous patients who told friends and colleagues that my practice was dedicated to cutting-edge technology. Some patients are referred without specific mention of laser cataract surgery, but rather are told that my practice is dedicated to technology and that I am a surgeon committed to innovation. While it is difficult to measure exactly how much my practice stands out due to my use of LenSx, it is clear to me that a residual effect of embracing high technology is improved reputation in my community.
Surgeons are responsible with their capital spends, and they correctly decline to purchase innovations that, even if impressive, do not generate a return on investment that justify the purchase price. In the case of LenSx, George et al found that only 8 to 13 FLACS procedures per month were needed to reach a break-even point at 5 years;13 they also found that the rate of premium IOL use increased by 23% during the first year of LenSx use.13 These data should be considered when weighing the potential of LenSx fitting into your practice.
CONCLUSION
After my initial experiences with LenSx, I asked myself a straightforward question: if a family member were undergoing cataract surgery, would I want them to have an experience that included LenSx? The answer was yes, and I promptly included LenSx technology in my surgical suite. Doing so gave me the confidence that my outcomes would be more predictable, empowering me to discuss premium IOL options with patients. This launched my practice to a new level, transforming my clinic into a refractive cataract practice rather than a routine cataract clinic.
If you’re aiming to improve your precision, efficiency, and outcomes, work with a platform with proven safety outcomes, and collaborate with an industry partner that offers effective support, then consider adopting LenSx technology in your practice.
1. Alcon Data on File, 2019.
2. Alcon Data on File, 2022.
3. Kohnen T, Mathys L, Petermann K, et al. Update on the comparison of femtosecond laser-assisted lens surgery to conventional cataract surgery: a systematic review and meta-analysis. Paper presented at: ESCRS; October 7-11, 2017; Lisbon, Portugal.
4. Kranitz K, Mihaltz K, Sandor GL, et al. Intraocular lens tilt and decentration measured by Scheimpflug camera following manual or femtosecond laser-created continuous circular capsulotomy. J Refract Surg. 2012;28(4):259-263.
5. Ali MH, et al. Comparison of characteristics of femtosecond laser-assisted anterior capsulotomy versus manual continuous curvilinear capsulorrhexis: a meta-analysis of 5-year results. J Pak Med Assoc. 2017;67(10):1574-1579.
6. Shajari M, et al. Comparison of 2 laser fragmentation patterns used in femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2017;43:1571-1574.
7. Zhang X, et al. Performance of femtosecond laser-assisted cataract surgery in Chinese patients with cataract: a prospective, multicenter, registry study. BMC Ophthalmol. 2019;19:7.
8. Yeu E, et al. A retrospective comparison of clinical outcomes associated with manual and femtosecond laser cataract surgery. Paper presented at: ASCRS; May 5-9, 2017; Los Angeles, CA.
9. Yeoh R. Practical differences between 3 femtosecond phaco laser platforms. J Cataract Refract Surg. 2014;40(3):510.
10. Nagy Z. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009;25(12):1053-1060.
11. Roberts HW, Wagh VK, Mullens IJM, et al. Evaluation of a hub-and-spoke model for the delivery of femtosecond laser-assisted cataract surgery within the context of a large randomised controlled trial. Br J Ophthalmol. 2018;102(11):1556-1563.
12. Alcon. LenSx Sales Aid. The LenSx® Laser facilitates personalized procedures. 2022 Alcon Inc. 12/22 US-LSX-2200024.
13. George DS, Ainsile-Garcia MH, Ferko NC, Cheng H. Successful implementation of femtosecond laser-assisted cataract surgery: a real-world economic analysis. Clin Ophthalmol. 2021;15:923-929.

Important Product Information
LENSX® LASER IMPORTANT PRODUCT INFORMATION FOR CATARACT SURGERY, CORNEAL FLAP AND CORNEAL POCKETS & TUNNEL INCISIONS
CAUTION: Federal Law restricts this device to sale and use by or on the order of a physician or licensed eye care practitioner.
INDICATIONS FOR THE LENSX® LASER: In the creation of corneal cuts/incisions (single-plane, multi-plane and arcuate) anterior capsulotomy and laser phacofragmentation during cataract surgery in adult patients. Each of these procedures may be performed either individually or consecutively during the same surgery.
CORNEAL FLAP INDICATION: For use in the creation of a corneal flap in adult patients undergoing LASIK surgery or other treatment requiring initial lamellar resection of the cornea.
CORNEAL POCKETS AND TUNNELS: In adult patients, for the creation of corneal pockets for placement/insertion of a corneal inlay device; and for creation of corneal tunnels for the placement of corneal rings.
RESTRICTIONS: Patients must be able to lie flat and motionless in a supine position. Patient must be able to understand and give an informed consent. Patients must be able to tolerate local or topical anesthesia. Patients with elevated IOP should use topical steroids only under close medical supervision.
CONTRAINDICATIONS
CATARACT SURGERY CONTRAINDICATIONS: Corneal disease that precludes applanation of the cornea or transmission of laser light at 1030 nm wavelength. Descemetocele with impending corneal rupture. Presence of blood or other material in the anterior chamber. Poorly dilating pupil, such that the iris is not peripheral to the intended diameter for the capsulotomy. Conditions which would cause inadequate clearance between the intended capsulotomy depth and the endothelium (applicable to capsulotomy only). Previous corneal incisions that might provide a potential space into which the gas produced by the procedure can escape. Corneal thickness requirements that are beyond the range of the system. Corneal opacity that would interfere with the laser beam, Hypotony, glaucoma* or the presence of a corneal implant. Residual, recurrent, active ocular or eyelid disease, including any corneal abnormality (for example, recurrent corneal erosion, severe basement membrane disease). History of lens or zonular instability. Any contraindication to cataract or keratoplasty. This device is not intended for use in pediatric surgery.
*Glaucoma is not a contraindication when these procedures are performed using the LenSx® Laser SoftFit® Patient Interface Accessory
CORNEAL SURGERY (FLAPS, POCKETS, TUNNELS) CONTRAINDICATIONS: Corneal lesions. Corneal edema. Hypotony. Glaucoma. Existing corneal implant. Keratoconus. This device is not intended for use in pediatric surgery. Flap creation, tunnels, pockets and cataract procedures cannot be combined into a single treatment.
WARNINGS: The LenSx® Laser System should only be operated by a physician trained in its use. The LenSx® Laser delivery system employs one sterile disposable Patient Interface consisting of an applanation lens and suction ring. The Patient Interface is intended for single use only. Use of disposables other than those manufactured by Alcon may affect system performance and create potential hazards.
PRECAUTIONS: Do not use cell phones or pagers of any kind in the same room as the LenSx® Laser. Discard used Patient Interfaces as medical waste.
COMPLICATIONS
CATARACT SURGERY AES/COMPLICATIONS: Corneal edema. Capsulotomy, phacofragmentation, or cut or incision decentration. Incomplete or interrupted capsulotomy, fragmentation, or corneal incision procedure. Capsular tear. Corneal abrasion or defect. Pain. Infection. Bleeding. Damage to intraocular structures. Anterior chamber fluid leakage, anterior chamber collapse. Elevated pressure to the eye.
CORNEAL SURGERY (FLAPS, POCKETS & TUNNELS) AES/COMPLICATIONS: Corneal edema. Corneal or eye pain. Corneal haze. Epithelial in-growth. Corneal abrasion or epithelial defect. Infection/keratitis. Corneal ectasia or endothelial perforation. Decentered flap or pattern; uneven flap bed. Incomplete dissection/inability to complete procedure. Flap tearing or incomplete lift-off. Free cap or buttonhole. Elevated pressure to the eye.
ATTENTION: Refer to the LenSx® Laser Operator’s Manual for a complete listing of indications, warnings and precautions.
VERION® IMAGE GUIDED SYSTEM IMPORTANT PRODUCT INFORMATION VERION® REFERENCE UNIT AND VERION® DIGITAL MARKER
CAUTION: Federal (USA) law restricts this device to sale by, or on the order of, a physician
INTENDED USES: The Verion® Reference Unit is a preoperative measurement device that captures and utilizes a high-resolution reference image of a patient’s eye. In addition, the Verion® Reference Unit provides pre-operative surgical planning functions to assist the surgeon with planning cataract surgical procedures. The Verion® Reference Unit also supports the export of the reference image, preoperative measurement data, and surgical plans for use with the Verion® Digital Marker and other compatible devices through the use of a USB memory stick. The Verion® Digital Marker links to compatible surgical microscopes to display concurrently the reference and microscope images, allowing the surgeon to account for lateral and rotational eye movements. In addition, details from the Verion® Reference Unit surgical plan can be overlaid on a computer screen or the physician’s microscope view.
CONTRAINDICATIONS: The following conditions may affect the accuracy of surgical plans prepared with the Verion® Reference Unit: a pseudophakic eye, eye fixation problems, a non-intact cornea, or an irregular cornea. In addition, patients should refrain from wearing contact lenses during the reference measurement as this may interfere with the accuracy of the measurements. The following conditions may affect the proper functioning of the Verion®
Digital Marker: changes in a patient’s eye between preoperative measurement and surgery, an irregular elliptic limbus (e.g., due to eye fixation during surgery, and bleeding or bloated conjunctiva due to anesthesia). In addition, the use of eye drops that constrict sclera vessels before or during surgery should be avoided.
WARNINGS: Only properly trained personnel should operate the Verion® Reference Unit and Verion® Digital Marker. Use only the provided medical power supplies and data communication cable. Power supplies for the Verion® Reference Unit and the Verion® Digital Marker must be uninterruptible. Do not use these devices in combination with an extension cord. Do not cover any of the component devices while turned on. The Verion® Reference Unit uses infrared light. Unless necessary, medical personnel and patients should avoid direct eye exposure to the emitted or reflected beam.
PRECAUTIONS: To ensure the accuracy of Verion® Reference Unit measurements, device calibration and the reference measurement should be conducted in dimmed ambient light conditions. Only use the Verion® Digital Marker in conjunction with compatible surgical microscopes.
ATTENTION: Refer to the user manuals for the Verion® Reference Unit and the Verion® Digital Marker for a complete description of proper use and maintenance of these devices, as well as a complete list of contraindications, warnings and precautions.
Trademarks are property of their respective owners.
© 2023 Alcon Inc. 3/23 US-LSX-2300008