
Although fortunately not a common occurrence, LASIK can induce aberrations in some eyes. The reason this phenomenon occurs is not entirely clear, but risk factors include preexisting corneal aberrations and irregularities in corneal hydration. Of course, inhomogeneity of the excimer laser beam itself can also produce an uneven treatment. Whatever the cause, once the complication has occurred in a patient who paid out of pocket for surgery to improve his or her visual function, he or she is bound to be disappointed with the outcome.
Topography-guided laser treatment has been available outside of the United States for more than 20 years, but the FDA issued its first approval of a topography-guided procedure in 2013: Contoura Vision (Alcon). At present, the procedure’s only approved indications are for the treatment of myopia and myopia with astigmatism. Topography-guided PRK (TG-PRK) shows promise, however, as a means by which to address LASIK-induced aberrations (off-label indication).
CASE EXAMPLE
A 75-year-old man presented to my practice. The patient had undergone bilateral LASIK many years earlier, followed by cataract surgery. After cataract surgery, the patient underwent excimer laser ablation to treat residual refractive error in his left eye.
Approximately 1 year later, he presented to my office with a complaint of significant blur, glare, and multiple images in the left eye. His UCVA was 20/50, and his BCVA was 20/25 with a refraction of -2.50 +0.50 x 30º. He reported ghosting and multiple images even with that correction in place.
Based on the patient’s subjective symptoms and the results of topography and aberrometry (Figures 1-3), I felt that he had developed irregular astigmatism (higher-order aberrations) in his left eye. In light of my success using Contoura Vision for virgin corneas, I decided to use the technology off-label for TG-PRK in this case. My initial goal was to retain some intermediate vision (-1.50 D) in his left eye. A surgical plan was developed based on topographic and aberrometry measurements (Figure 4). Because the ablation pattern mimics a hyperopic ablation (peripheral annular treatment that would increase the amount of postoperative myopia), I attempted to compensate by adding a myopic treatment.
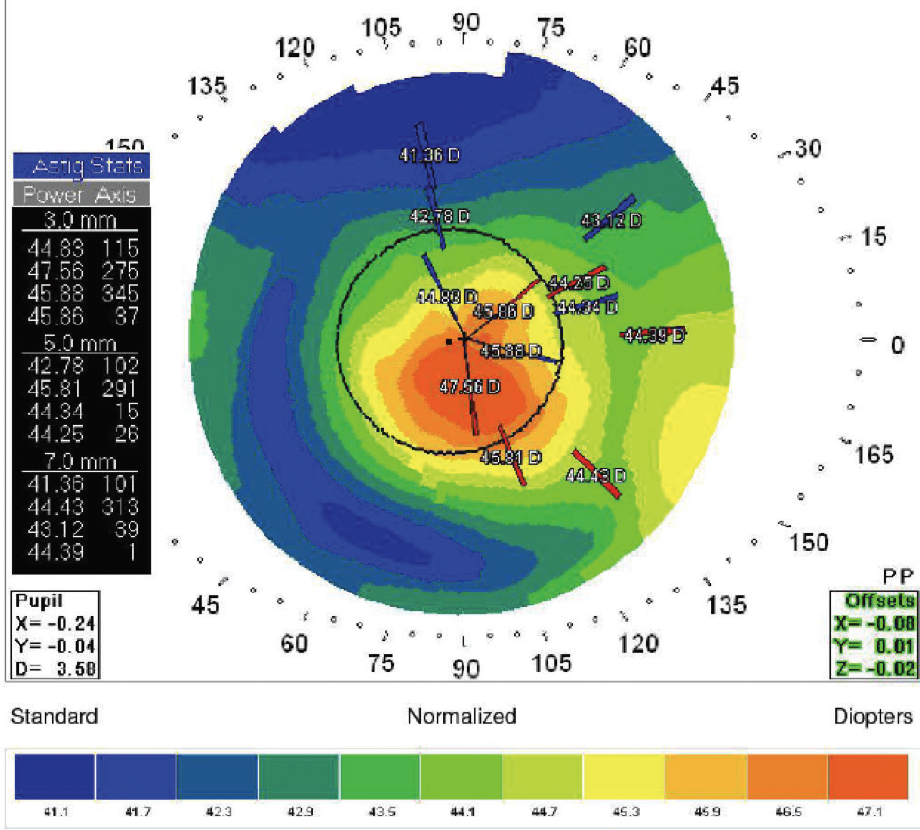
Figure 1. Placido topography of the patient’s left eye.
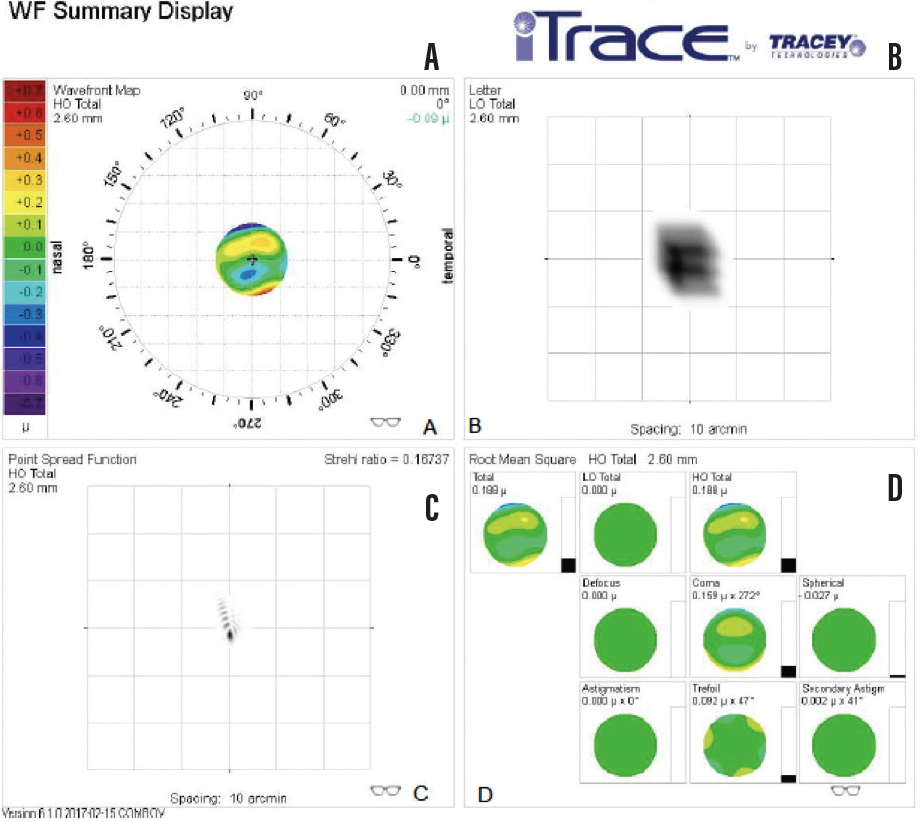
Figure 2. Aberrometry of the left eye shows increased coma (A and D) and an abnormal point spread function (C).
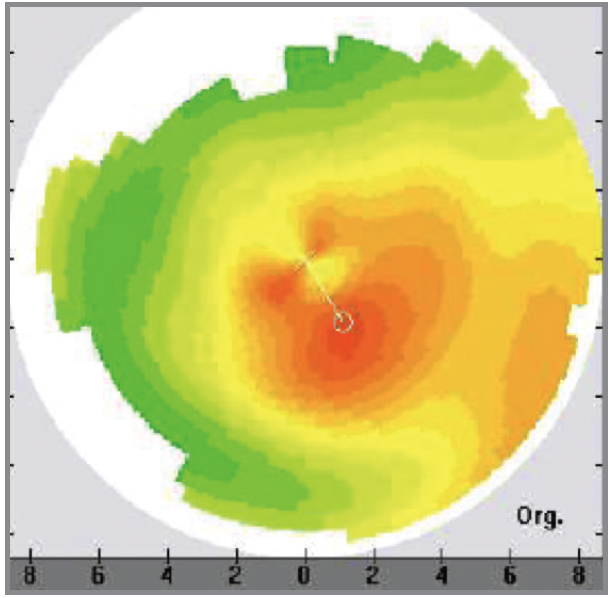
Figure 3. Topography of the left eye shows central irregularity.
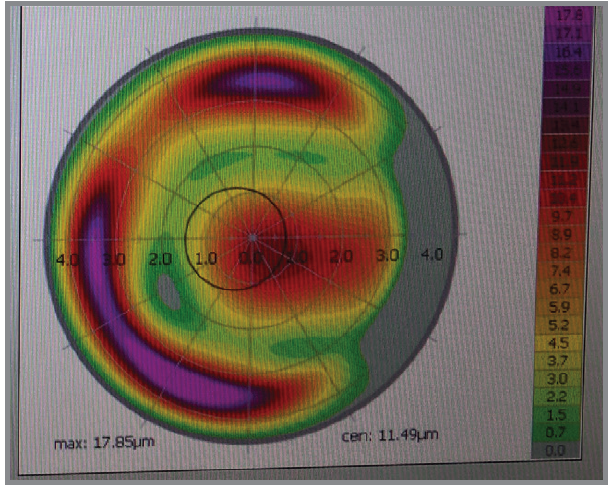
Figure 4. Treatment pattern with Contoura Vision shows a peripheral annular ablation plan.
The patient’s refractive result was a little too good: I had overcompensated for the hyperopic ablation, leaving him with a plano refraction (20/20+2 UCVA) instead of -1.50 D. He has maintained this result for the past 11 months. Fortunately, despite having excellent uncorrected distance VA instead of uncorrected intermediate VA, he is extremely pleased with the result because of the almost complete resolution of his higher-order aberrations (Figure 5).
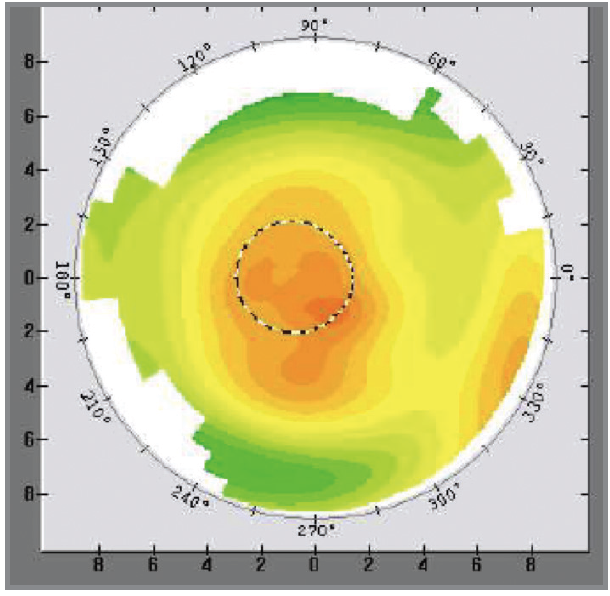
Figure 5. Topography after the TG-PRK procedure. Compared with Figure 3, the central cornea shows much greater homogeneity.
Take-Home Points
- A wavefront-guided laser treatment measures irregularities in the lens, optical media, and cornea. In contrast, topography-guided PRK (TG-PRK) measures and treats aberrations on the corneal surface, which demands the reproducible capture of corneal topographic and aberrometric data. It is exceedingly important that the ocular surface be healthy when measurements are obtained. I also instruct patients to discontinue wearing their contact lenses for 2 weeks before preoperative measurements. The TG-PRK procedure corrects both lower- and higher-order aberrations.
- The first step in determining who is a candidate for TG-PRK is corneal analysis with an aberrometer. The second step is to incorporate the measurements into the topography-guided laser system in order to construct a surgical plan that can correct the aberrations that were identified.
- When using TG-PRK to treat patients with corneal aberrations, the goal is to address their debilitating symptoms, not necessarily to achieve 20/20 VA. It is also important to understand that the topography-guided correction of certain higher-order aberrations induced by LASIK can often mimic a hyperopic ablation, which can leave patients slightly more myopic. Surgeons often attempt to compensate, but residual ametropia may be expected. With appropriate preoperative counseling, many patients are happy to wear glasses or contact lenses in exchange for relief from seeing multiple images, glare, streaking, and/or halos. Alternatively, a nontopography-guided procedure may be performed once the refraction has stabilized.
- When a LASIK procedure induces optical aberrations, it is important for surgeons to acknowledge what the patient is seeing. A key step in the healing process is for the surgeon to sit down with the patient and say that, although LASIK typically achieves excellent results, the current outcome is less than ideal. Next, the surgeon can outline the potential solutions.
- Obtaining useful measurements, analyzing the results, and adjusting the TG-PRK treatment to account for this information can be challenging. It is highly beneficial for surgeons interested in this type of laser vision correction to find a mentor who has a lot of experience with TG-PRK and who is willing advise them. Most of these individuals will be located outside of the United States, where the procedure has been available for much longer. As US surgeons gain experience, they can help each other achieve excellent results in these difficult cases.



