




Our understanding of the role of Demodex has expanded in recent years, including our knowledge of Demodex blepharitis, where inflammation is caused by overpopulation of Demodex mites in the eyelash follicles. Demodex blepharitis is quite common, accounting for about 45% of blepharitis cases.1 It’s particularly common among older patients, including 84% of people age 60 and older,2 but it also affects younger people, particularly those with rosacea3 or immune system challenges such as diabetes.4 The problem is so widespread that when 1,121 sequential patients in multiple eye care practices were screened for collarettes, a pathognomonic sign of Demodex blepharitis, it was found in 58% of patients.5 If we extrapolate that 58% to the adult population in our clinics, it’s possible that 25 million Americans have Demodex blepharitis.
With these numbers in mind, it is clear that Demodex is “hiding in plain sight” among our current patients. Screening is essential because if we treat Demodex blepharitis without addressing the Demodex infestation specifically, then mites will continue to proliferate, and the condition will worsen.
Thankfully, screening is quite fast and simple. During the slit-lamp examination, we have the patient look down, and we look for collarettes around the lashes on the upper lid. Collarettes—the accumulated debris and waste of Demodex mites living in the lash follicles—indicate the presence of Demodex mites 100% of the time.6 Because collarettes offer positive identification of Demodex blepharitis, there is no need to pluck an eyelash and examine it microscopically. We also do not need to rely on patients’ symptoms to guide us, which is advantageous because symptoms of Demodex blepharitis often don’t correlate with signs, particularly in the elderly population. One of my case studies is just such a patient.
Treating Demodex Blepharitis
While identifying Demodex blepharitis is simple, treatment can be a challenge. Off-label treatments are not proven. Some treatment options have limited success, but they don’t fully control Demodex and may even cause further damage to the delicate eyelid tissues.
For example, tea tree oil lid scrubs can help control the Demodex population, but they can also be very harsh and irritating, and the traumatic mechanical scrubbing can cause lash loss. Also, new evidence finds that terpinen-4-ol, a tea tree oil component, is toxic to meibomian gland epithelial cells, even in low concentrations.7 In-office blepharoexfoliation is deeper and more effective than at-home lid scrubs, but the mechanical process is not specific to Demodex and does not kill the mites. Plus, patients must pay for blepharoexfoliation every few months, and the device requires an investment from the practice. In the following two cases, I was able to improve Demodex blepharitis with the treatments at our disposal, but they were limited in their efficacy, tolerability, and compliance.
Case 1: 72-Year-Old Man
A 72-year-old man presented for cataract surgery and told me, “Doctor, I want to get rid of my glasses!” He said that his vision was getting worse at the end of the day, especially after reading or watching television. But when I asked how his eyes were feeling, he said they felt fine. The examination showed that his best corrected VA was 20/40 OD and 20/50 OS, and he had 2+ nuclear sclerotic cataracts in both eyes.
Despite reporting that his eyes felt comfortable, the patient had 2+ central punctate keratitis with staining and a tear breakup time of 2-3 seconds in both eyes. I noted 1+ meibomian gland dysfunction, as well as significant collarettes along the lash base on both eyes, demonstrating Demodex blepharitis (Figure 1).

Figure 1. This 72-year-old man presented for cataract surgery, however Demodex blepharitis, evidenced by collarettes, MGD, and abnormal TBUT, led us to delay surgery.
The patient declined to have blepharoexfoliation treatment for the Demodex blepharitis because he didn’t feel that anything was wrong. After discussion and education, including an explanation of how his problem would increase the risk for infection and complications after cataract surgery, he agreed to postpone cataract surgery and initiate some blepharitis treatments. He began using tea tree oil commercial lid scrubs and a tea tree oil face wash, as well as regular hot compresses and preservative-free artificial tears.
After 6 weeks of aggressive tea tree oil lid scrubs, we were able to proceed with cataract surgery. Postoperatively, the patient developed more significant symptoms of ocular surface disease, including morning stickiness of lids, redness, and foreign body sensation in both eyes. I told him to continue using his tea tree oils scrubs and face wash, as well as his compresses and tears. Unfortunately, the patient was very noncompliant with his lid hygiene instructions. He feels that cataract surgery has made his eyes feel more irritated and uncomfortable than ever, and he is very unhappy.
Case 2: 24-Year-Old Woman
A 24-year-old software engineer was experiencing recurrent chalazia and chronic/recurrent stye formation in both eyes. Wearing her soft contact lenses resulted in rapid redness and irritation, so she stopped. With a career that involved many hours in front of the computer, her gritty, irritated eyes and red eyelids were making it difficult to work.
The examination showed that the patient’s BCVA was 20/20 in both eyes. She had a small chalazion on the left upper eyelid and diffuse collarettes along the upper and lower lash base, indicating Demodex blepharitis (Figure 2). Meibomian gland expression revealed a slow secretion of thickened meibum. To address the Demodex blepharitis, she was treated in the office with blepharoexfoliation of all four eyelids. She started on a commercial tea tree oil lid scrub twice a day and tea tree oil face wash. She also began doing regular hot compresses on her eyes to thin her meibum secretions, as well as using preservative-free artificial tears.
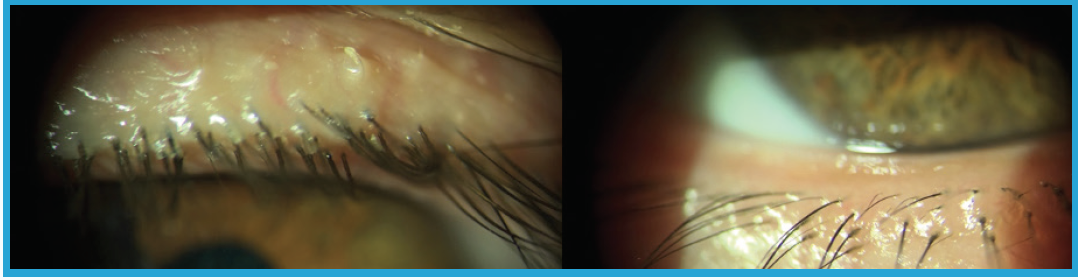
Figure 2. This 24-year-old woman presented with a small chalazion on the left upper eyelid (left). On slit-lamp examination, diffuse collarettes were evident along the upper and lower lash base (right), telling us that she had Demodex blepharitis.
After 1 month, the patient was able to have some symptomatic relief from blepharoexfoliation and the recommended management. Her busy life makes it difficult to keep up with twice-daily lid scrubs, but she continues to come in every 3-4 months for blepharoexfoliation treatment. Oral doxycycline and topical cyclosporin have produced only minimal improvement in her symptoms. She still feels frustrated by chronic and recurrent symptoms of Demodex blepharitis that impact her quality of life and cosmetic appearance. She cannot work comfortably, wear her soft contact lenses for more than a few hours, or wear makeup.
Promising Treatment Pipeline for Demodex Blepharitis
These patients showed some improvement, but we did not achieve full resolution of their Demodex blepharitis. It’s clear that compliance with irritating, inconvenient lid scrubs is a major barrier to even modest success, and we need a treatment that is proven safe and effective. I’m very excited about new, targeted therapeutics in the pipeline designed to address Demodex blepharitis at the root cause. As we identify more people with this “hidden” problem, we may soon be able to provide better patient care and thus have happier patients.
1. Zhao YE, Wu LP, Hu L, et al. Association of blepharitis with Demodex: a meta- analysis. Ophthalmic Epidemiol. 2012;19(2):95-102.
2. Liu J, Sheha H, Tsenga SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010; 10(5): 505–510. Available at: https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC2946818/. Accessed: November 3, 2020.
3. Zhang XB, Ding YH, He W. The association between demodex infestation and ocular surface manifestations in meibomian gland dysfunction.Int J Ophthalmol. 2018;11(4):589-592. Available at: https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC5902361/. Accessed: November 3, 2020.
4. Yamashita LS, Cariello AJ, Geha NM, et al. Demodex folliculorum on the eyelash follicle of diabetic patients. Arq Bras Oftalmol. 2011;74(6):422-424. Available at: https://www.scielo.br/scielo.php?script=sci_arttext&pid =S0004-27492011000600008. Accessed: November 3, 2020.
5. Tarsus Collarette Prevalence Study. 2020.
6. Gao YY, Di Pascuale MA, Li W, et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci. 2005;46(9):3089-3094.
7. Chen D, Wang J, Sullivan DA, et al. Effects of terpinen-4-ol meibomian gland epithelial cells in vitro. Cornea. 2020.
