


Prospective Multicenter Trial of a Small-Aperture Intraocular Lens in Cataract Surgery

Dick HB, Piovella M, Vukich J, Vilupuru S, Lin L; Clinical Investigators1
Industry support: Study supported by AcuFocus
ABSTRACT SUMMARY
This European prospective surgical trial was conducted at 12 clinics in Austria, Belgium, Germany, Italy, Spain, and Norway. Investigators studied the clinical acceptability of unilateral implantation of a small-aperture IOL (IC-8, AcuFocus, not available in the United States) followed by the contralateral implantation of an aspheric monofocal IOL.
STUDY IN BRIEF
In a multicenter clinical trial, implanting a small-aperture IOL (IC-8, AcuFocus, not available in the United States) in one eye and an aspheric monofocal IOL in the contralateral eye produced good visual outcomes and high patient satisfaction. As with other premium IOL technologies, patient selection requires careful consideration, and patients should be educated about lifestyle and vision requirements as a way of setting reasonable expectations. Patients who require sharp intermediate and near visual acuity and those who have irregular pupils because of iris trauma are good candidates for a small-aperture IOL.1
WHY IT MATTERS
Clinicians already knew that implanting a small-aperture IOL in one eye and a monofocal IOL in the fellow eye can provide a continuous broad range of vision and excellent visual acuity across all focal distances. This study showed that targeting a small amount of myopia (-0.75 D) in the eye with the small-aperture IOL can extend the range of functional near vision by 1.00 D without compromising uncorrected distance visual acuity.
1. Souza CE, Muccioli C, Soriano ES, et al. Visual performance of AcrySof Restor apodized diffractive IOL: a prospective comparative trial. Am J Ophthalmol. 2006;141(5):827-832.
The IC-8 is a one-piece hydrophobic acrylic IOL with a centrally located embedded annular mask designed to improve near visual acuity based on the concept of small-aperture optics. The embedded annular mask has an outer diameter of 3.23 mm and a central aperture of 1.36 mm (Figure).
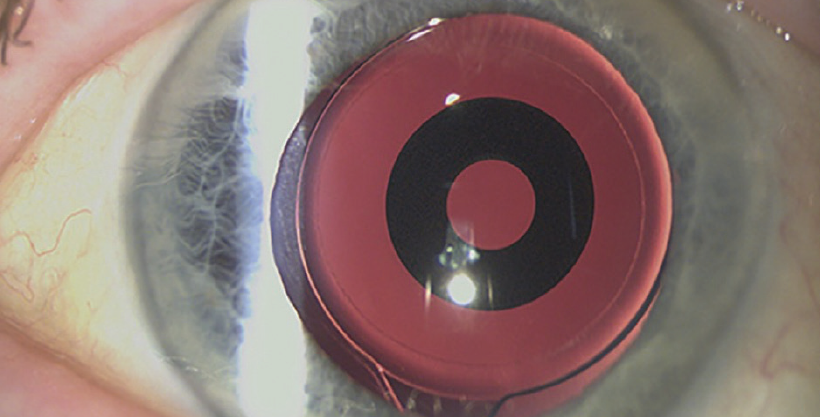
Figure. An IC-8 small-aperture IOL in situ.
The study included 105 patients. The follow-up period was 6 months. The investigators assessed postoperative uncorrected near visual acuity (UNVA), uncorrected intermediate visual acuity (UIVA), uncorrected distance visual acuity (UDVA), depth of focus, contrast sensitivity, patient satisfaction, visual symptoms, and adverse events.
Postoperatively, eyes that received the small-aperture IOL had mean uncorrected Snellen visual acuities of 20/23 UDVA, 20/24 UIVA, and 20/30 UNVA. Binocular UDVA, UIVA, and UNVA was 20/32 or better in 99%, 95%, and 79% of patients, respectively. Ninety-three patients (95.9%) stated that they would undergo the procedure again, and four patients (4.1%) stated that they would not.
The investigators reported that visual performance, safety, patient satisfaction, and their tolerance of residual astigmatism were all excellent 6 months after implantation of the small-aperture IOL.
DISCUSSION
Multifocal and trifocal IOLs provide good functional vision, but results with these modalities are limited by reduced contrast sensitivity, visual disturbances, and a noncontinuous range of vision.2-5 Better outcomes are achieved with bilateral implantation of trifocal or multifocal IOLs than with unilateral implantation.6-8
Implanting a small-aperture IOL in one eye and an aspheric monofocal IOL in the fellow eye is part of a binocular approach. The goal is to reduce the patient’s dependence on spectacles by extending the depth of focus from far through near in the eye with the small-aperture IOL and by providing good UDVA in the eye with a monofocal lens implant.
To optimize outcomes, these researchers recommend targeting a postoperative manifest refraction spherical equivalent of -0.75 D in the eye that receives a small-aperture IOL and plano in the eye that receives a monofocal IOL to improve the targeted corrected defocus curves.
Earlier studies have shown that patients who receive a small-aperture IOL can tolerate up to 1.50 D of astigmatism, whereas other research has found that astigmatism reduces the visual acuity of patients who receive multifocal IOLs.9,10
Small Aperture IC-8 Intraocular Lens in Cataract Patients: Achieving Extended Depth of Focus Through Small Aperture Optics
Hooshmand J, Allen P, Huynh T, et al11
Industry support: No
ABSTRACT SUMMARY
In this multicenter, nonrandomized, retrospective case series, 126 consecutive patients received an IC-8 IOL at six centers across Australia. Outcome measures were UDVA, UIVA at 80 cm, and UNVA at 40 cm. The researchers assessed adverse events (AEs), spectacle independence, visual symptoms, and patient satisfaction at the final follow-up visit. (No specific time frame was mentioned in the study.)
The AEs in this cohort included IOL explantation and exchange in seven patients (5.5%). Most of these AEs were attributed to poor visual acuity because of early posterior capsular opacification and uncertainty about whether an Nd:YAG laser posterior capsulotomy could be performed through an IC-8 lens. One patient had difficulty adjusting to the difference between the two eyes, and one patient underwent an IOL exchange for a monofocal IOL because of large floaters that developed after a posterior vitreous detachment. This patient did not notice any improvement in symptoms after the IOL exchange.
At the final follow-up visit, more than 50% of patients reported complete spectacle independence for distance, intermediate, and near visual activities. The other patients wore spectacles only for specific tasks such as hobbies that required near visual acuity and reading in dim light.
Study in Brief
For this multicenter retrospective case study, investigators compiled data on 126 patients undergoing bilateral cataract extraction who received a small-aperture IOL in one eye and a monofocal IOL in the fellow eye. At the final follow-up visit, more than 50% of patients reported complete spectacle independence for distance, intermediate, and near visual activities.
WHY IT MATTERS
In addition to providing important information about spectacle independence with the unilateral implantation of a small-aperture IOL, this study’s findings suggest that patients who would be considered poor candidates for multifocal IOLs because of preexisting ocular pathology may be suitable candidates for a small-aperture lens. Data on the quality of optical image focus for the IC-8 lens and a comparison with a monofocal IOL are published for the first time in this study.
The investigators concluded that the IC-8 IOL can provide extended depth of focus after cataract surgery, allowing 54% of patients to achieve complete spectacle independence for reading.
DISCUSSION
In multiple studies, the IC-8 has been found to provide superior depth of focus for UNVA and UIVA compared to monofocal and accommodating IOLs and results slightly better than or comparable to those of multifocal IOLs.1,12,13 The ability of this small-aperture IOL to deliver a high level of spectacle independence comes from a combination of:
1) Targeting a small amount of monovision (mini-monovision of approximately -0.75 D) in the eye that receives the IC-8 and emmetropia in the contralateral eye receiving a monofocal IOL and
2) The extended range of depth of focus provided by the IC-8 IOL (especially under photopic conditions).
Clinically, there were few drawbacks to the small-aperture IOL in this study. Only a small number of patients experienced lasting adverse visual effects that, in contrast, are often experienced by patients who receive multifocal IOLs.14,15 The dysphotopic symptoms that patients experienced were transient and usually resolved with neural adaptation.
The utility of this small-aperture IOL in the context of astigmatism was evident particularly in one patient with keratoconus. With 4.25 D of corneal cylinder and a UNVA of 6/19 postoperatively, the patient was “delighted” with the functional range of vision when on the job as a truck driver.
This case series included patients with preexisting ocular comorbidities that would be considered relative contraindications for the implantation of multifocal IOLs. These comorbidities included age-related macular degeneration, marked higher-order aberrations from corneal pathology, and epiretinal membranes. Although the number of such cases in the series was small, the investigators suggested that patients who would be considered unsuitable candidates for multifocal IOL implantation may be suitable candidates for an IC-8 lens.
1. Dick HB, Piovella M, Vukich J, Vilupuru S, Lin L; Clinical Investigators. Prospective multicenter trial of a small-aperture intraocular lens in cataract surgery. J Cataract Refract Surg. 2017;43(7):956-968.
2. Montés-Micó R, España E, Bueno I, Charman WN, Menezo JL. Visual performance with multifocal intraocular lenses: mesopic contrast sensitivity under distance and near conditions. Ophthalmology. 2004;111(1):85-96.
3. Gil MA, Varón C, Cardona G, Vega F, Buil JA. Comparison of far and near contrast sensitivity in patients symmetrically implanted with multifocal and monofocal IOLs. Eur J Ophthalmol. 2014;24(1):44-52. Published correction appears in Eur J Ophthalmol. 2015;25(6):575.
4. Chiam PJ, Chan JH, Aggarwal RK, Kasaby S. Restor intraocular lens implantation in cataract surgery: quality of vision. J Cataract Refract Surg. 2006;32(9):1459-1463. Published correction appears in J Cataract Refract Surg. 2006;32(12):1987.
5. de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859-865.
6. Kretz FT, Müller M, Gerl M, Gerl RH, Auffarth GU. Binocular function to increase visual outcome in patients implanted with a diffractive trifocal intraocular lens. BMC Ophthalmol. 2015;15:110.
7. Steinert RF, Aker BL, Trentacost DJ, Smith PJ, Tarantino N. A prospective comparative study of the AMO Array zonal-progressive multifocal silicone intraocular lens and a monofocal intraocular lens. Ophthalmology. 1999;106(7):1243-1255.
8. Cionni RJ, Osher RH, Snyder ME, Nordlund ML. Visual outcome comparison of unilateral versus bilateral implantation of apodized diffractive multifocal intraocular lenses after cataract extraction: prospective 6-month study. J Cataract Refract Surg. 2009;35(6):1033-1039.
9. Hayashi K, Hayashi H, Nakao F, Hayashi F. Influence of astigmatism on multifocal and monofocal intraocular lenses. Am J Ophthalmol. 2000;130(4):477-482.
10. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8):1323-1329.
11. Hooshmand J, Allen P, Huynh T, et al. Small aperture IC-8 intraocular lens in cataract patients: achieving extended depth of focus through small aperture optics. Eye (Lond). 2019;33(7):1096-1103.
12. Grabner G, Ang RE, Vilupuru S. The small-aperture IC-8 intraocular lens: a new concept for added depth of focus in cataract patients. Am J Ophthalmol. 2015;160:1176-1184.e1.
13. Ong HS, Evans JR, Allan BD. Accommodative intraocular lens versus standard monofocal intraocular lens implantation in cataract surgery. Cochrane Database Syst Rev. 2014;(5):CD009667.
14. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110(9):1789-1798.
15. Gil MA, Varon C, Cardona G, Vega F, Buil JA. Comparison of far and near contrast sensitivity in patients symmetrically implanted with multifocal and monofocal IOLs. Eur J Ophthalmol. 2014;24(1):44-52.

