
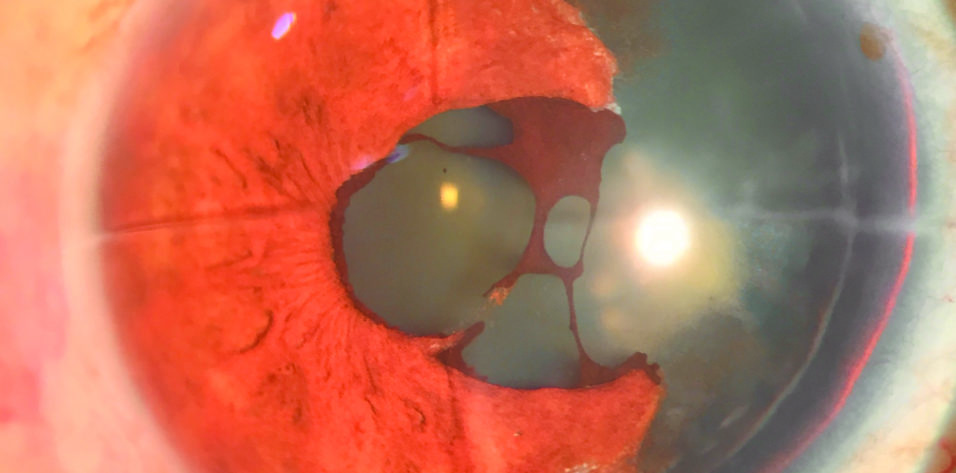
A 59-year-old man with a history of radial keratotomy (RK) in both eyes presented for a cataract evaluation (Figure 1). The patient stated that he had begun experiencing reduced vision, glare, and photophobia in his right eye 1 year earlier. Three years before presentation, the right eye sustained a closed-globe injury from a cricket ball; management was conservative.
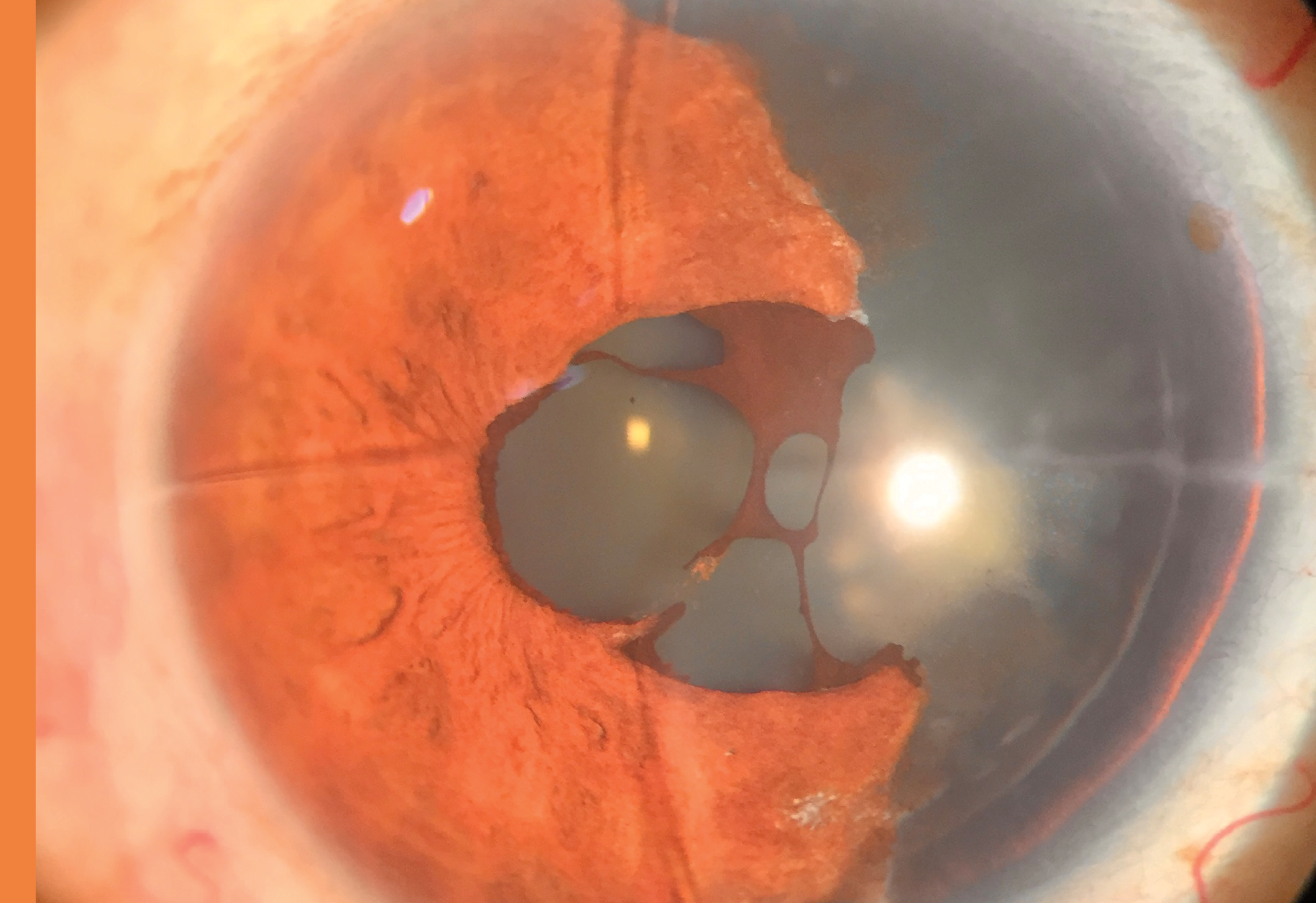
Figure 1. Partial aniridia and a nuclear cataract in the right eye of a patient with a history of RK.
On examination, the patient’s corrected distance visual acuity (CDVA) was 6/60 OD and 6/9 OS. Four RK incisions were visible in the cornea of each eye. Partial aniridia and a nuclear cataract were evident in the right eye. Gonioscopy found crumpled uveal remnants at the nasal angle of the right eye that were suggestive of iris tissue and no evidence of angle recession. The IOP was 12 mm Hg OU with Goldmann applanation tonometry. A posterior segment examination of each eye was normal.
The patient elected to undergo cataract surgery and the implantation of an iris reconstruction device in the right eye. He was counseled on his limited visual potential due to the aniridia and history of RK. The ASCRS IOL power calculator for prior RK and data obtained with the Atlas 9000 Corneal Topographer (Carl Zeiss Meditec), Pentacam HR (Oculus Optikgeräte), and IOLMaster 700 (Carl Zeiss Meditec) were used. We chose the maximum IOL power suggested and discussed the expected residual refractive error and postoperative regression to the patient.
Phacoemulsification was performed through a temporal posterior limbal incision to prevent the RK incisions from opening. After the implantation of a hydrophobic IOL (Tecnis Monofocal 1-Piece, model ZCB00, Johnson & Johnson Vision) in the bag, a 311 aniridia implant (Ophtec) was placed in the bag and rotated to the intended position. The postoperative drug regimen consisted of topical antibiotic and steroid drops in a tapering dose for 4 weeks.
Postoperatively, the patient’s CDVA was 6/9 with a residual refractive error of +1.25 D of sphere and +0.75 D of cylinder (Figure 2). The photophobia and glare had decreased significantly compared to preoperative levels. Pre- and postoperative studies with the iTrace (Tracey Technologies) demonstrated a significant improvement in aberrations (Figure 3). The iris prosthesis rotated slightly after surgery, but no intervention was performed because the patient was satisfied with the visual outcome (Figure 4).
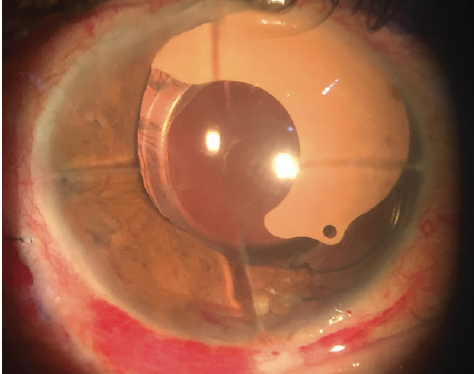
Figure 2. The IOL in the bag and the artificial iris device 1 day after surgery.
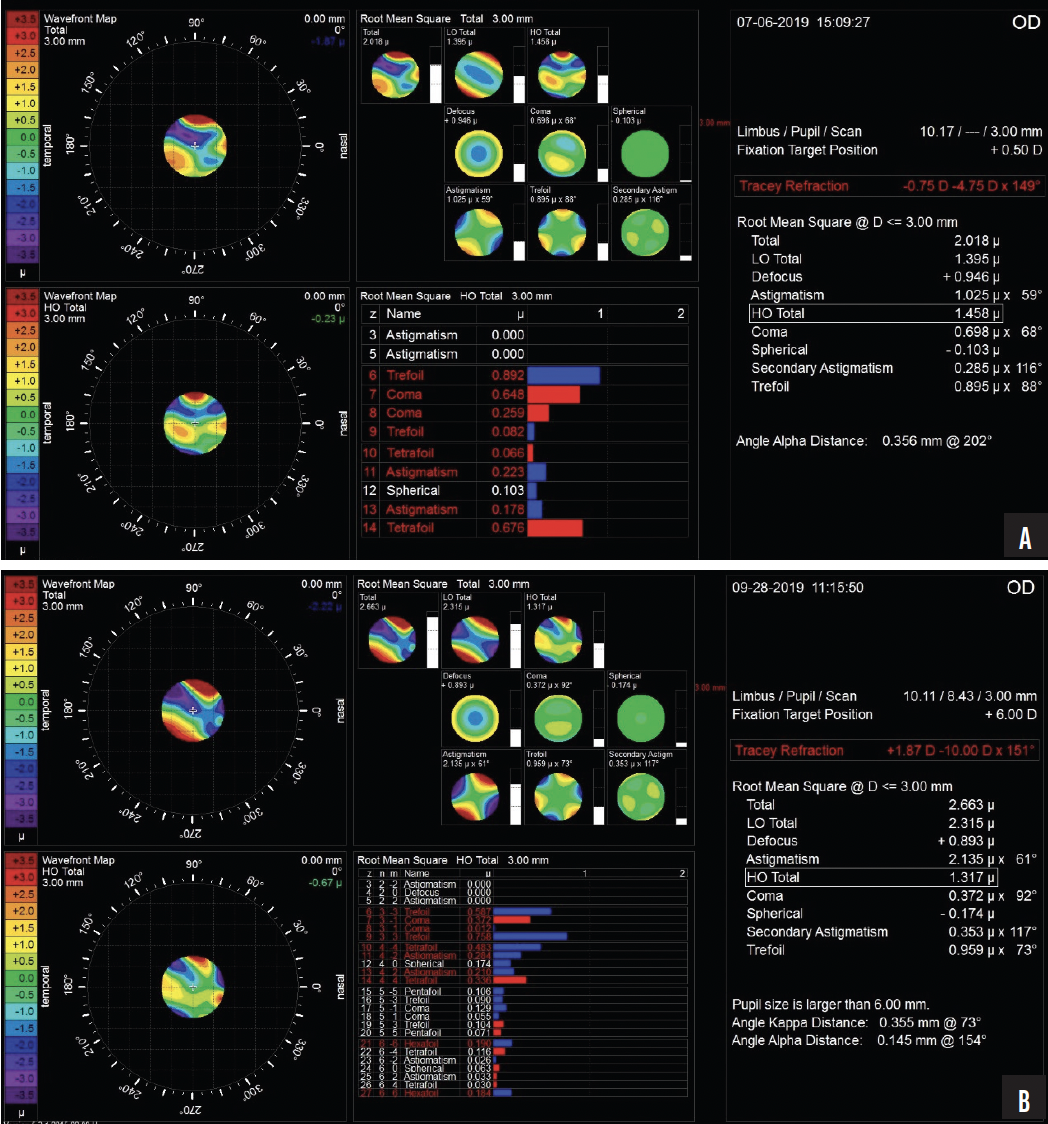
Figure 3. Pre- (A) and postoperative (B) aberration profiles with the iTrace.
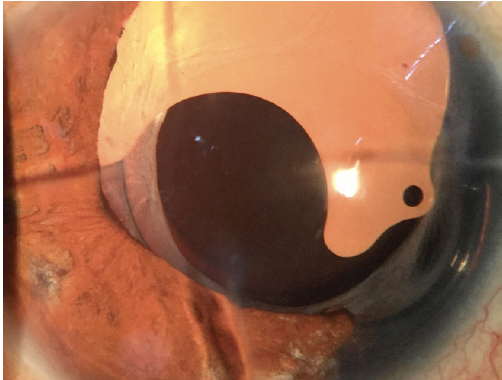
Figure 4. The eye 3 months after surgery.
DISCUSSION
In expulsive iridodialysis or traumatic aniridia, the iris is torn completely from the ciliary body. This clinical condition usually occurs after a severe contusion to the eye.1 Partial aniridia can be corrected by the simultaneous implantation of a foldable IOL and artificial iris.2
Wang et al3 reported improved CDVA in a case series of 38 eyes that received the 311 aniridia implant. A limitation of the device is that it is available in only three colors, and patients should be informed preoperatively of the cosmetic implications. We have found the device useful for correcting aberrations due to aniridia and RK scars.
1. Yang H, Liu CJL. Traumatic aniridia with extensive episcleral pigmentation: a case report. BMC Ophthalmol. 2022;22:60.
2. Forlini C, Forlini M, Rejdak R, et al. Simultaneous correction of post-traumatic aphakia and aniridia with the use of artificial iris and IOL implantation. Arch Clin Exp Ophthalmol. 2013;251(3):667-675.
3. Wang H, Jung J, Lin SR, Olson MD, Miller KM. Safety and efficacy of colored iris reconstruction lens implantation. Am J Ophthalmol. 2020;216:174-185.

