


Dr. Buonsanti levitates a luxated IOL from the posterior chamber, exchanges it for a three-piece IOL, and sutures one haptic to the iris in an eye with a small pupil and a history of vitrectomy.
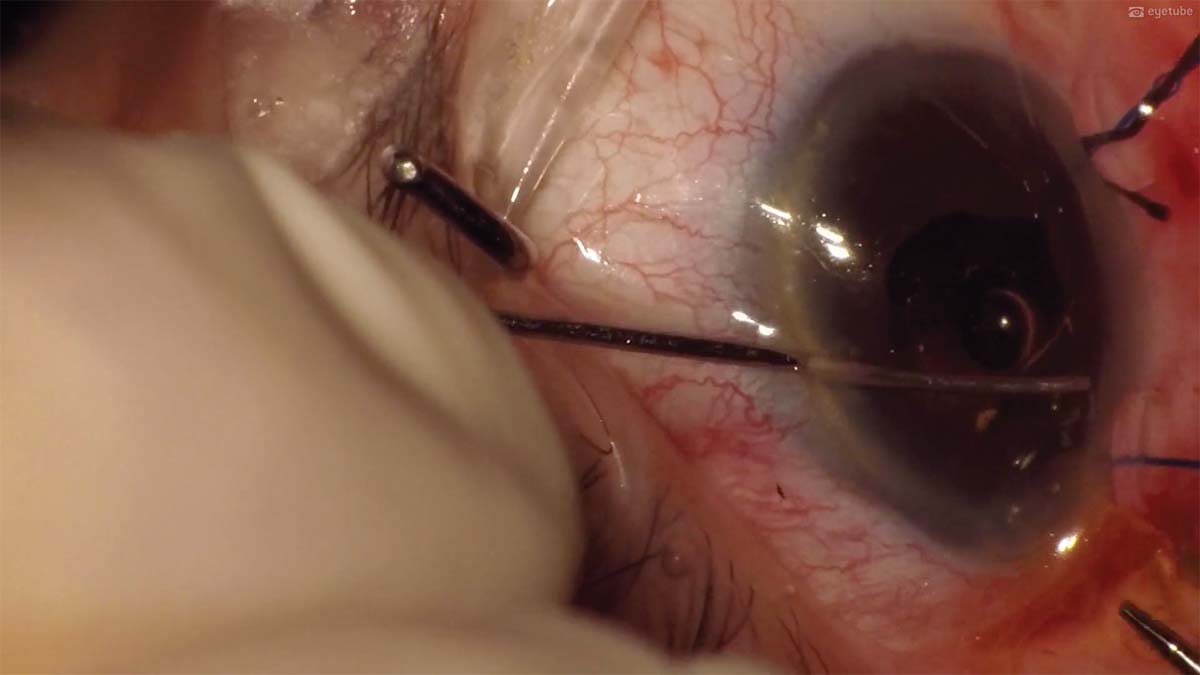
1. A 73-year-old woman reports experiencing blurred vision in her right eye after lifting a heavy object. The eye has a small pupil. In the right eye, the patient underwent a pars plana vitrectomy 20 years ago and cataract surgery with implantation of a one-piece acrylic toric IOL in the sulcus 3 years ago. A posterior capsular break occurred during cataract surgery. The IOL is not visible, even with a 90.00 D lens. If the patient looks up and down quickly, however, one haptic is visible near the pupil. It is clear that the IOL has dropped right behind the iris. There is no vitreous traction. The sideport incisions are created. The pupil is then stretched with two Buonsanti Dual Hooks (Madhu Instruments)—a combination iris retractor/capsular hook device—by using the end with the iris retractor.
2. An OVD is injected into the anterior chamber. A 30-gauge needle is used to lift the dropped IOL, which is then grasped with microforceps. The IOL has completely subluxated in the anterior chamber.
3. A 3.0-mm main incision is created with a diamond blade, and a bolus of OVD is injected into the anterior chamber to protect the endothelium.
4. The IOL is cut in half. A spatula is inserted through the sideport incision to prevent the IOL from touching the endothelium while being explanted.
5. The original IOL is removed through the main incision, and a three-piece acrylic hydrophobic IOL is implanted in the sulcus.
6. The Buonsanti Dual Hooks are removed.
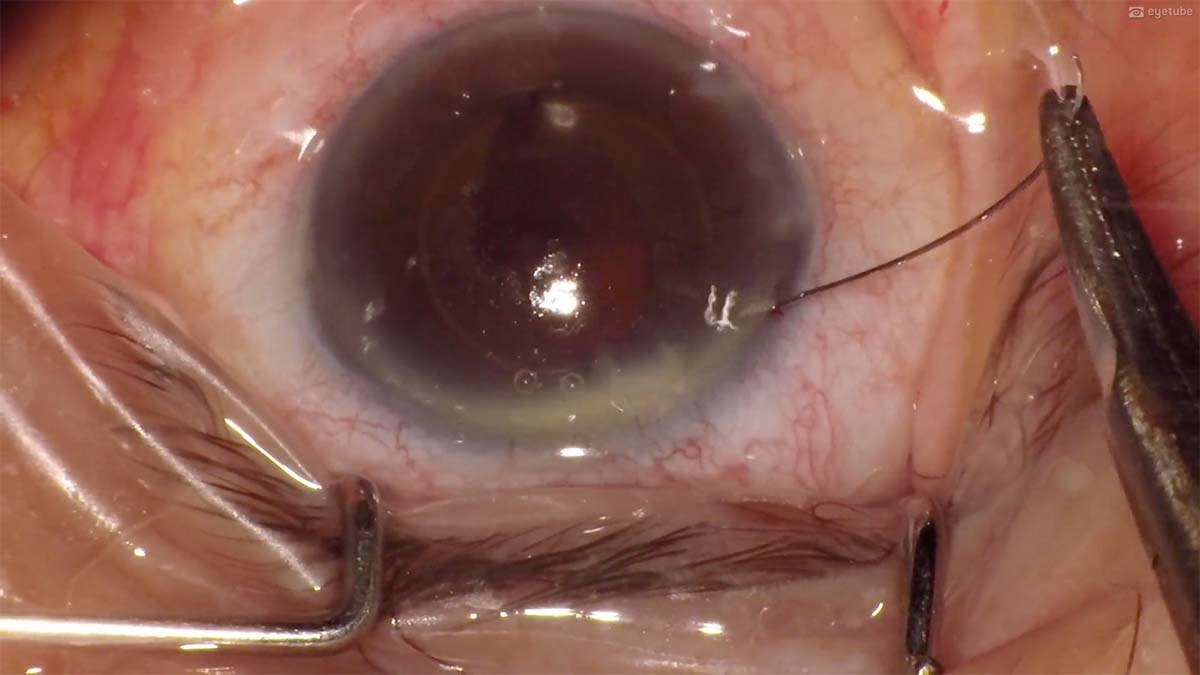
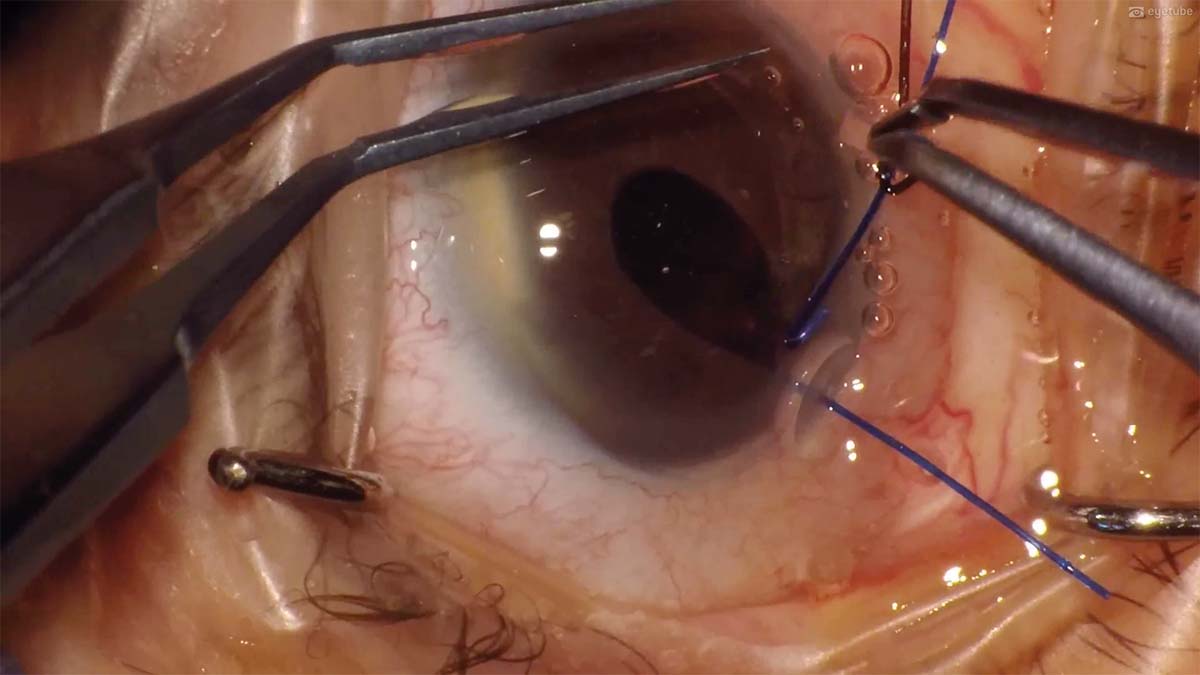
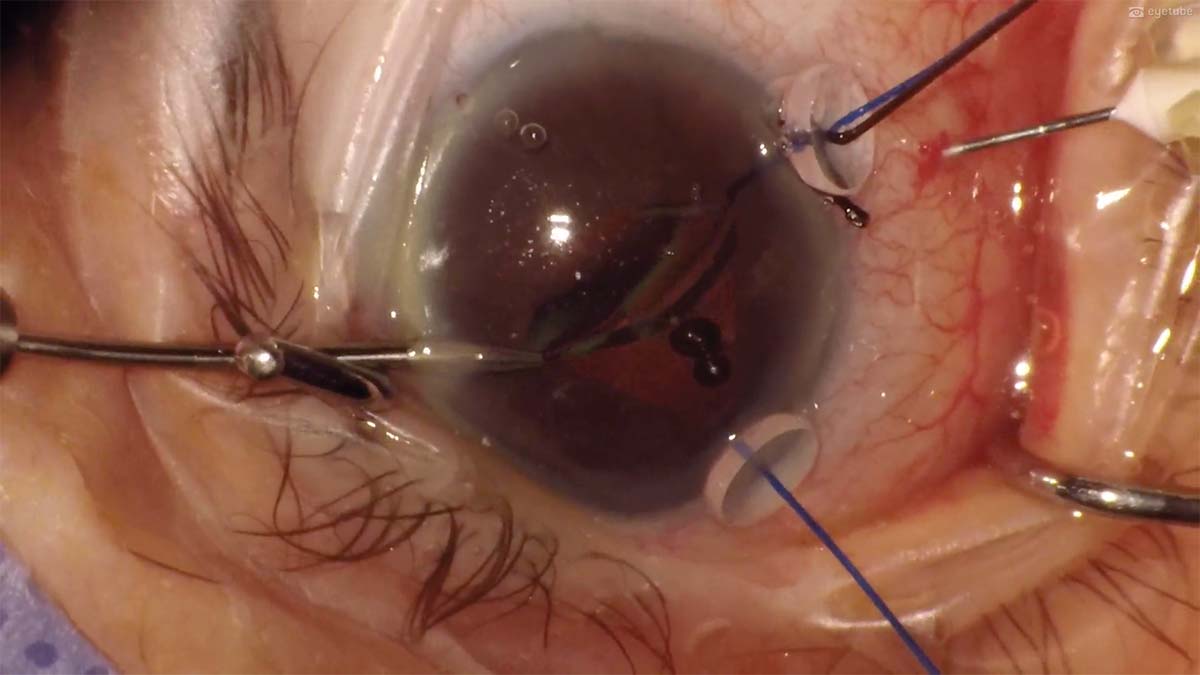
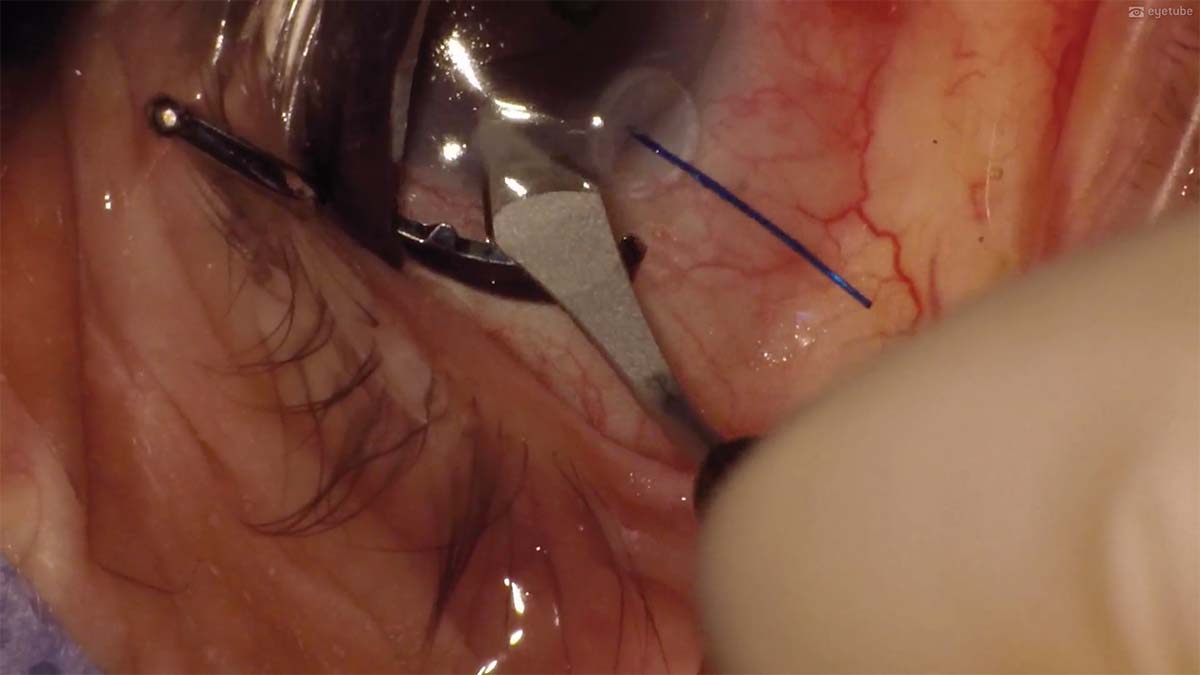
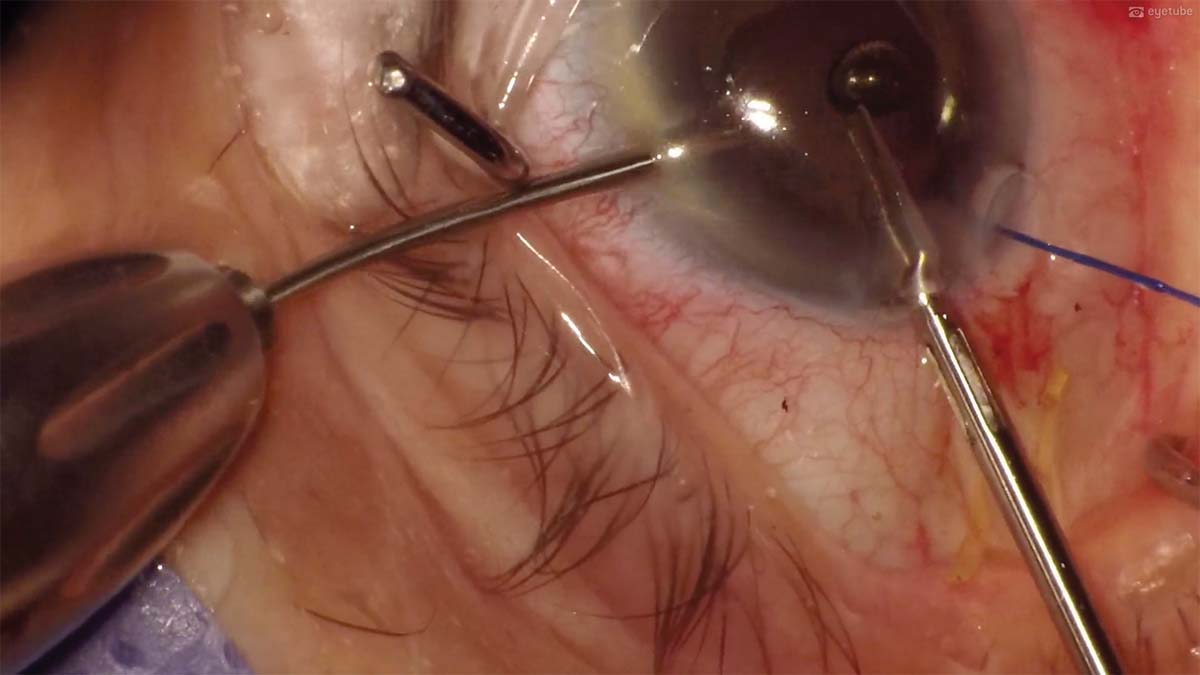
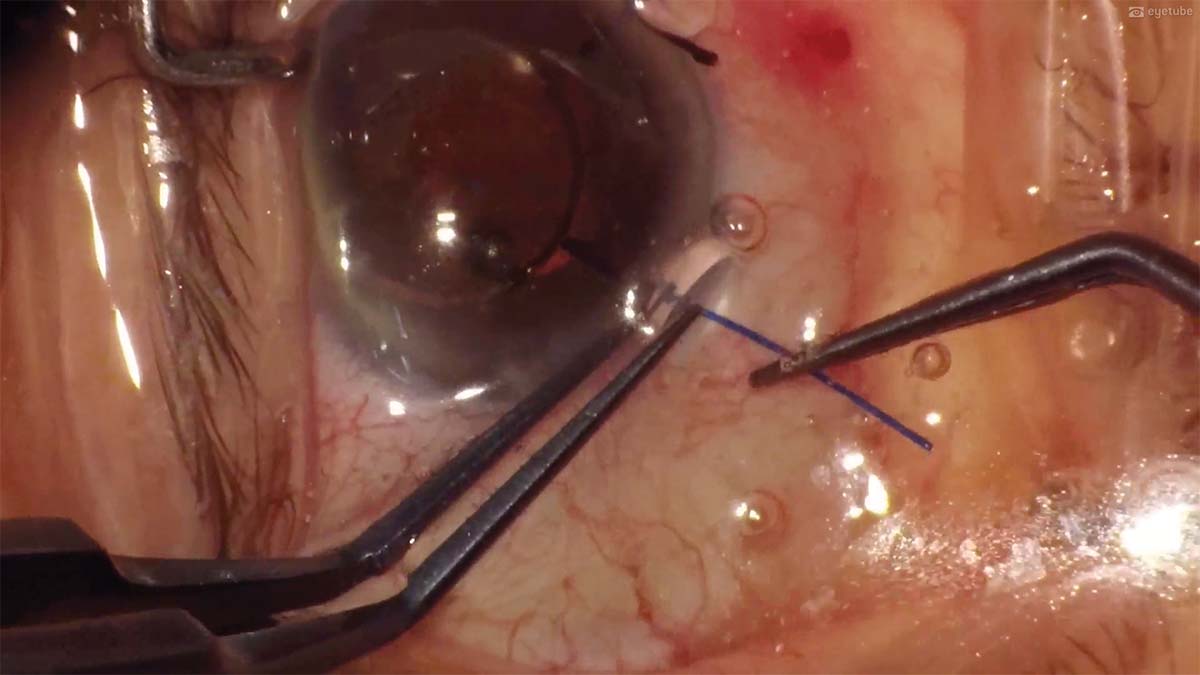
7. Because the superior rim of the anterior lens capsule is unstable, the superior IOL haptic is sutured to the iris. A paracentesis is made, and a 10-0 polypropylene (Prolene, Ethicon) suture is passed through the iris, behind the superior haptic, and out through the iris again. At the end of the case, the IOL is well centered.
Honorable Mentions
No. 1 | Transscleral Fixation Using a Combination of Six Techniques
Ma’an Albarry, MD, FRCS
Dr. Albarry details the advantages of six techniques he used to perform transscleral fixation of a monofocal IOL in an aphakic vitrectomized eye.
No. 2 | Traumatic Cataract With 4 Clock Hours of Iridodialysis and Zonulysis
John Philip Lim, MD
Dr. Lim explains how he managed a traumatic cataract in a 22-year-old patient who was in a motor vehicle accident.
No. 3 | Good to Bad and Back Again
Jason Jones, MD
Dr. Jones performs several maneuvers to remove the nucleus and cortex successfully after the vitreous prolapses early in the course of routine cataract surgery.


