



The COVID-19 pandemic has been a major learning experience. It has transformed the practice of medicine from shutdown to delivering care through telemedicine to a new normal. This pandemic led me to change my practice in ways I’d never thought about. My staff and I established processes that have improved patient safety and care as well as the efficiency of care delivery. Our highest priority, however, remains the patient experience.
INCREASED INTEREST
I have a boutique practice on the Gulf Coast of Florida. My surgical volume was 20% higher in the first quarter of this year compared to the same period in 2020 (we missed 8 weeks of surgery in 2020). Comparing these same periods, my premium conversions are up by about 2%. Even though this is not a significant change, what is significant is that many more patients are coming into the office since we resumed offering surgery after the shutdown to inquire about certain types of IOLs. For many of them, foggy spectacle lenses from wearing masks is the driver; they desire greater independence from glasses. They are using their increased free time to research their options and then asking questions about the pros and cons of premium IOLs. Some patients have even requested IOLs that are not currently available in the United States. These experiences demonstrate the importance of keeping our practice’s website and our approach to premium IOLs current.
Patients are also more frequently requesting an upgrade to laser cataract surgery. Approximately 85% to 87% of my patients choose laser cataract surgery as an upgrade. Limited travel plans have left many of them with more disposable income, and they are willing to spend that money on themselves. Further, Florida is a hot spot for retirees; we see our community growing larger each year.
This trend in patient upgrades spurred me to take a closer look at how my practice approaches premium conversions.
PREOPERATIVE CONSULTATION
The examination. Each patient’s surgical experience starts and ends with me. During the examination, I discuss all of the pathology that I find. Retinal or macular issues are addressed, even if it means referring the patient to a specialist for a consultation.
Problems with the eyelids and corneal surface are discussed. My staff and I bear in mind the following saying: If patients didn’t know they had dry eye before surgery, then the surgery caused it. Approximately 70% of my patients have dry eye disease that requires treatment. At the preoperative visit, ocular surface disease treatment, including hypochlor spray, fluorometholone acetate ophthalmic suspension 0.1% (Flarex, Eyevance Pharmaceuticals), and/or preservative-free tears, all administered twice daily, is initiated, and patients are scheduled to return for diagnostic testing and surgical counseling.
Surgical counseling. My surgical counselor stays abreast of the latest technology so that she can educate patients about their cataract journey and help to identify the type of IOL best suited to them. I review patients’ medical records with the diagnostic technician and the surgical counselor before diagnostic testing is performed. Information on patients’ pathology and my recommendations guide the counselor in identifying which type of IOL to recommend.
During the consultation, the surgical counselor begins by sharing a menu that starts with basic surgery. Each surgical elective—from the use of intraoperative aberrometry to the premium lens package—is explained fully. Reviewing the different surgical procedures and lenses helps put into perspective the outcome patients can expect.
The counselor then asks what goal patients hope to obtain and shows patients their diagnostic results as visual aids to help explain the reasons for the recommendations. Most patients have talked to their friends and relatives about their experiences with cataract surgery, so it is important for the counselor to emphasize that no two eyes are identical and therefore not all surgeries and outcomes are alike. Patients are also informed that all IOLs have limitations. We make a point to underpromise and overdeliver.
An uptick in our premium IOL conversion rate presents other unique opportunities, including offering patients nonsurgical aesthetic care (see Aesthetic Opportunity).
Aesthetic Opportunity
Many patients who elect to receive premium IOLs no longer wear glasses and therefore can’t hide behind them, so to speak. A large proportion of them return to the office to tell me that their eyelids look droopy and/or that their eyes are not as white or bright as they used to be. In response, I recently began offering oxymetazoline hydrochloride ophthalmic solution 0.1% (Upneeq, RVL Pharmaceuticals). This topical medication raises the upper eyelids an average of 1 to 2 mm for 8.3 hours (ie, the half-life of Upneeq; data on file with RVL Pharmaceuticals). My patients are experiencing amazing results without undergoing cosmetic surgery, and they are commenting that the whites of their eyes are brighter from this treatment (Figure).
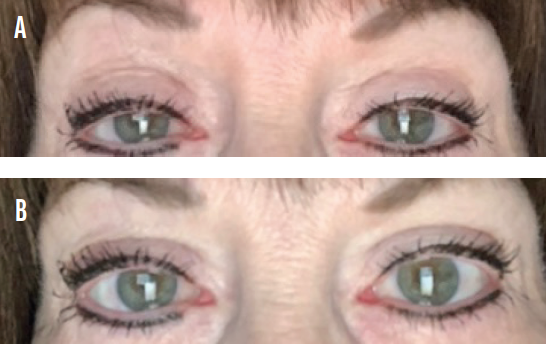
Figure. Before (A) and after (B) treatment with oxymetazoline hydrochloride ophthalmic solution 0.1%.
CONCLUSION
Despite the rollout of COVID-19 vaccines, my staff and I are not relaxing our safety protocols. We continue to ask patients to remain in their cars until they are called to enter the office for their appointments. Physical distancing requirements have been maintained in the waiting area. Patients and staff are required to wear masks while in the office, surfaces are disinfected after each patient visit, and the door is opened and closed for patients as they enter and exit the office. Our patients thank us for the care we take to keep them safe, and they appreciate the efforts we take to educate them on their options.

